Endoscopic ultrasound procedures represent a significant component of gastroenterology and oncology practices, yet many providers struggle with proper coding and billing for these services. Understanding the correct eus cpt code assignment is essential for accurate reimbursement and compliance with payer requirements. Medical billing professionals must navigate multiple code options, each representing distinct procedural variations and anatomical considerations. Proper code selection directly impacts revenue capture and reduces the risk of claim denials or audits.
Understanding EUS Procedure Codes
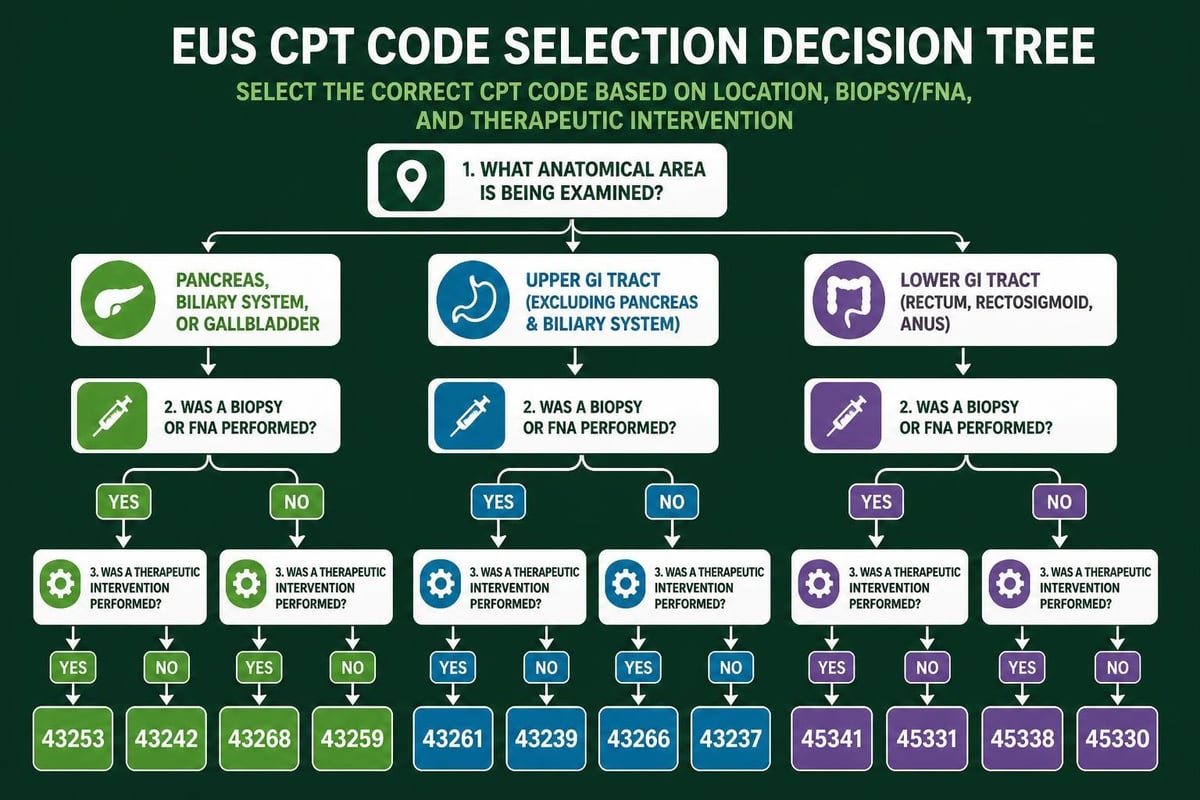
The eus cpt code family encompasses several distinct codes, each representing specific procedural elements and anatomical regions examined. CPT code 43259 describes esophagogastroduodenoscopy with endoscopic ultrasound examination, covering the esophagus, stomach, and either the duodenum or surgically altered stomach. This comprehensive code requires complete examination of multiple anatomical regions to justify billing.
Another frequently utilized code is CPT 43242, which covers endoscopic ultrasound-guided fine needle aspiration or biopsy of the upper gastrointestinal tract. This code specifically addresses diagnostic sampling procedures that combine imaging guidance with tissue acquisition. Understanding when each code applies prevents revenue leakage and ensures compliant billing practices.
Key Code Distinctions
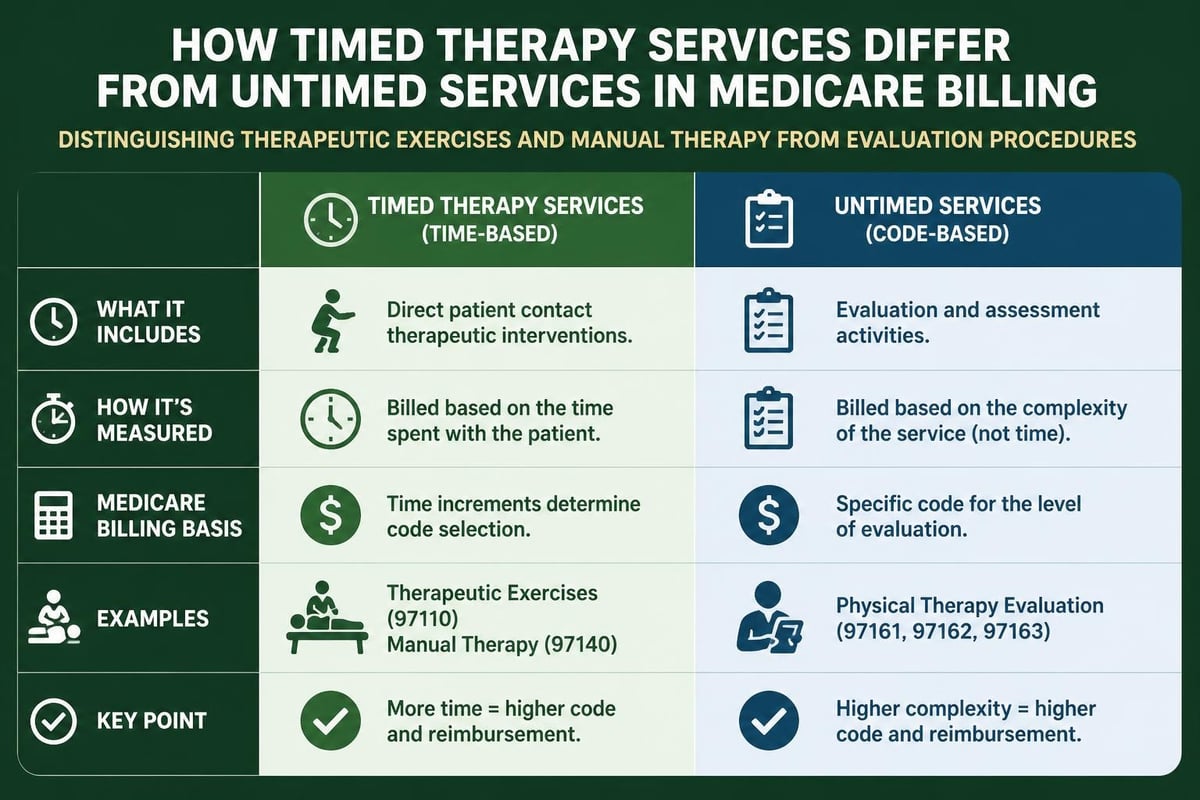
Medical billing specialists must recognize the critical differences between diagnostic and therapeutic EUS procedures. Diagnostic codes cover examination and visualization, while therapeutic codes include interventional elements such as:
- Fine needle aspiration for tissue sampling
- Drainage procedures for fluid collections
- Celiac plexus neurolysis for pain management
- Pseudocyst drainage with stent placement
- Vascular structure assessment and intervention
Each procedural variation requires specific documentation elements to support the selected code. The National Cancer Institute defines EUS as a procedure combining endoscopy with ultrasound to create detailed images of the digestive tract and surrounding tissues, emphasizing its dual diagnostic capability.
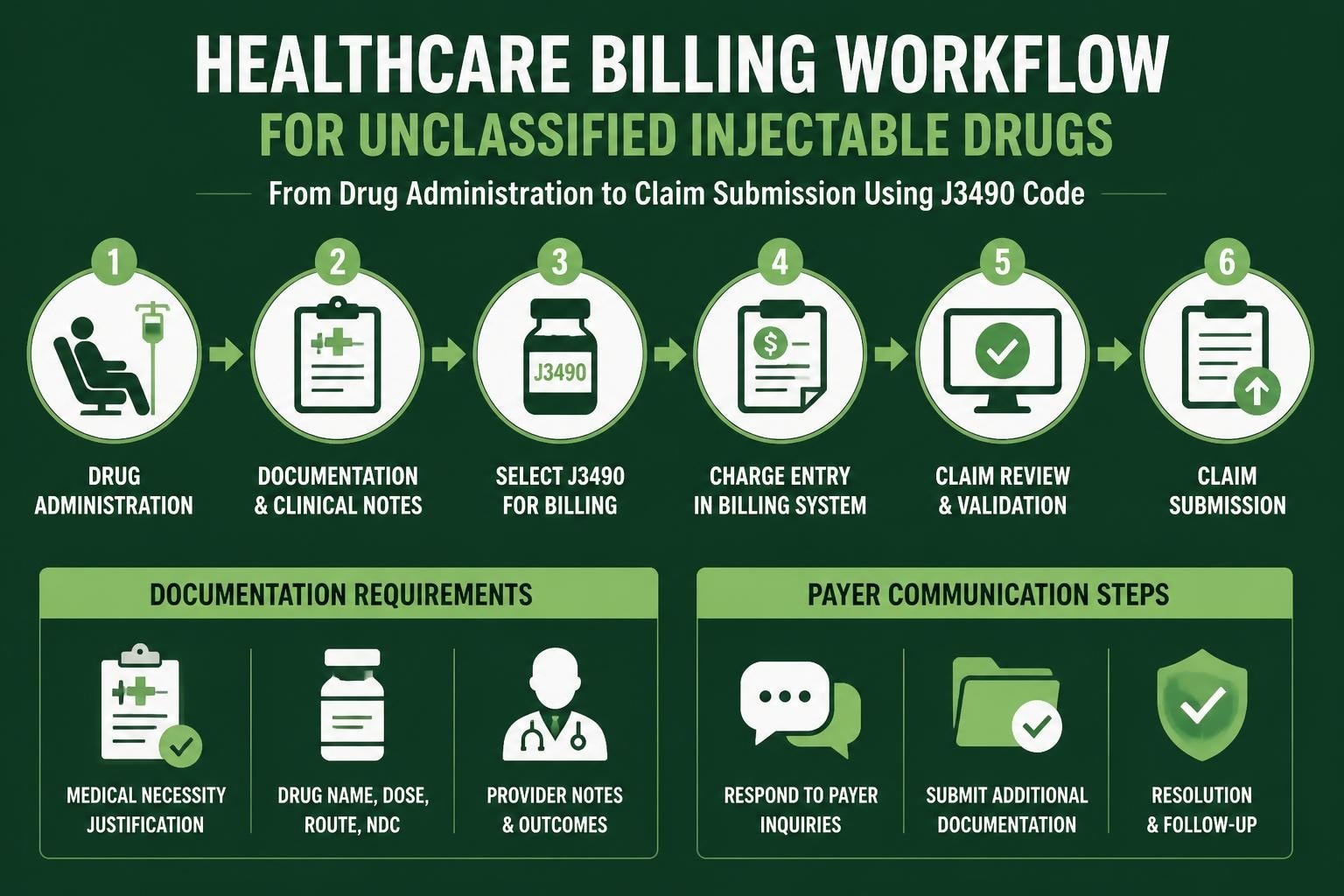
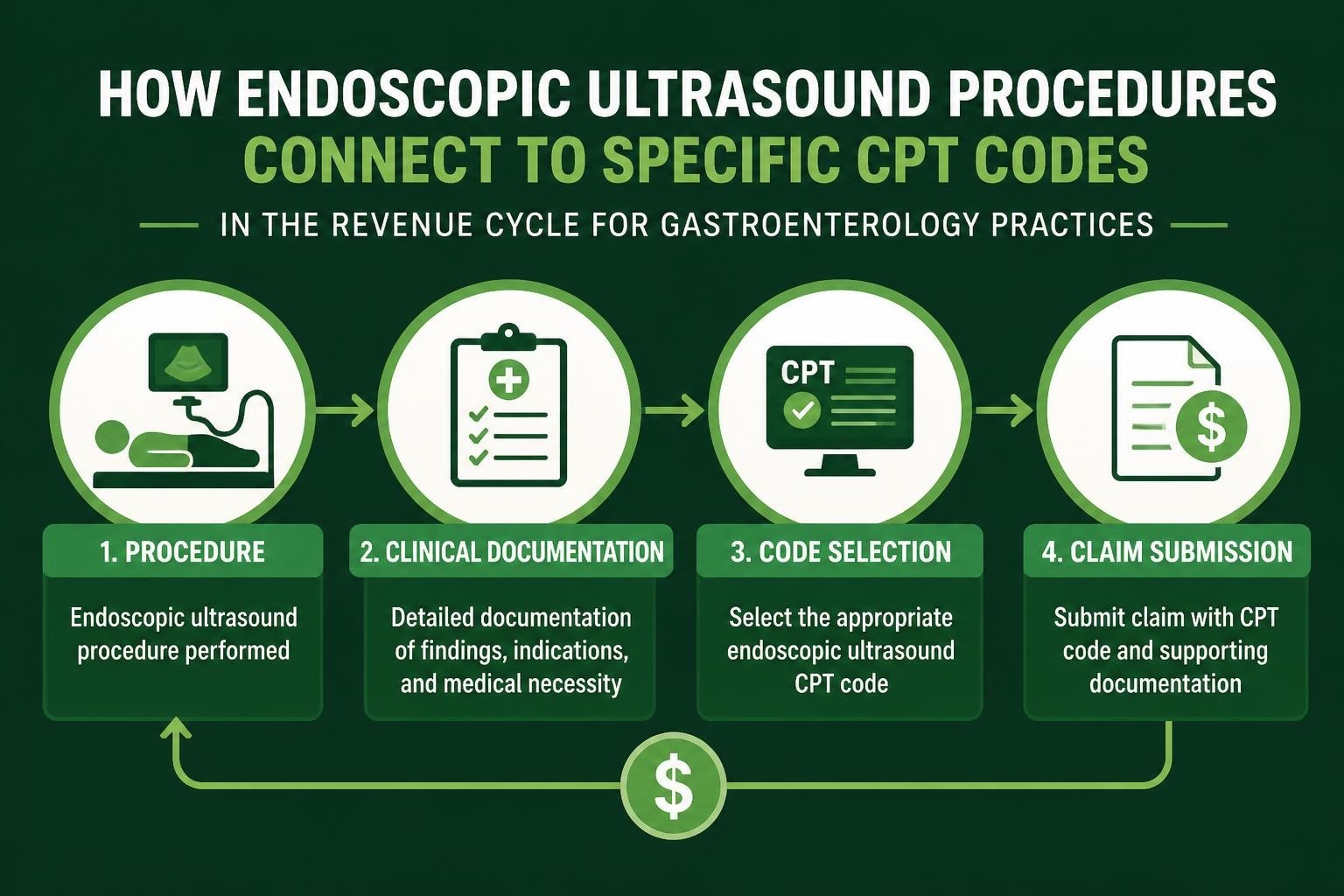
Documentation Requirements for EUS Billing
Complete and accurate documentation forms the foundation of successful EUS claims processing. Providers must document specific elements to justify the eus cpt code selected and demonstrate medical necessity. Insufficient documentation represents one of the primary causes of claim denials in gastroenterology practices.
| Documentation Element | Required Details | Common Deficiencies |
|---|---|---|
| Indication | Medical necessity rationale | Vague or missing clinical justification |
| Anatomical regions | All areas examined with findings | Incomplete regional documentation |
| Equipment specifications | Endoscope type, ultrasound frequency | Missing technical parameters |
| Procedural details | Step-by-step narrative | Generic template language |
| Pathology correlation | Biopsy results when applicable | Lack of follow-up documentation |
Practices should implement standardized documentation templates that prompt providers to include all necessary elements. However, templates must allow sufficient flexibility for individualized patient details rather than generic, pre-populated language that suggests lack of actual examination.
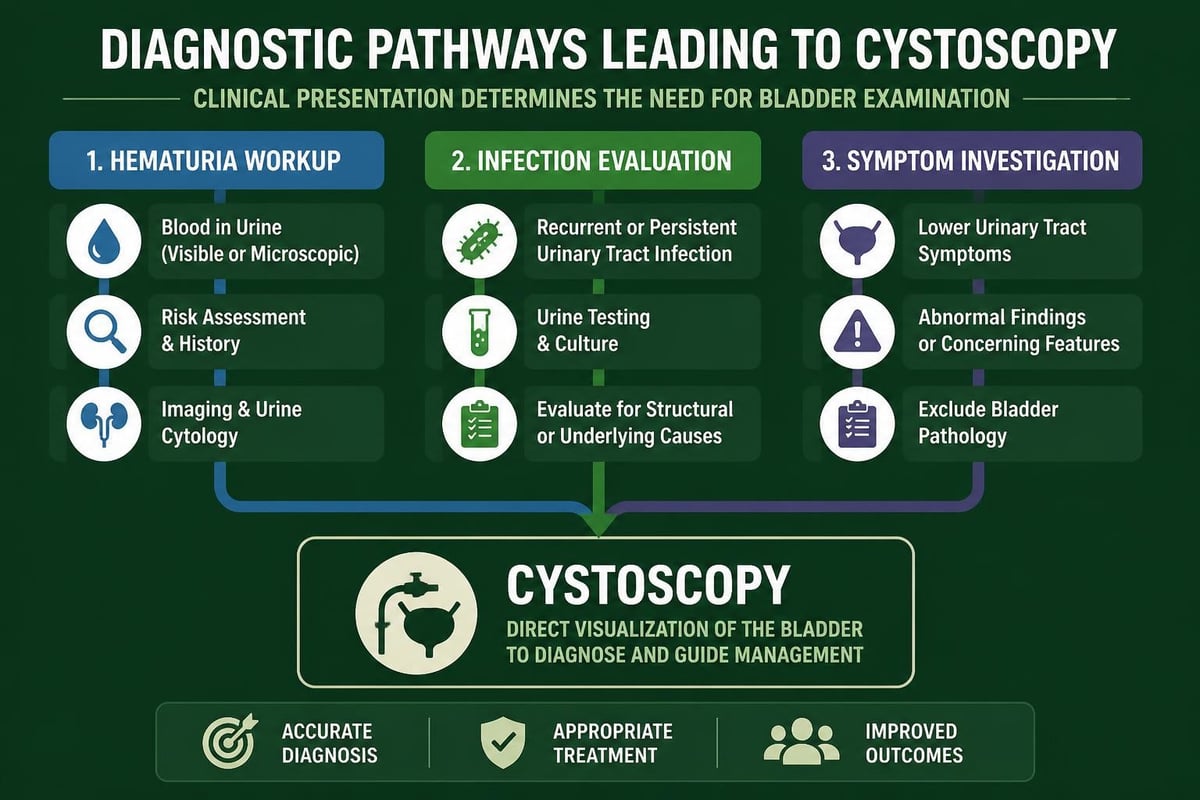
Medical Necessity Considerations
Payers scrutinize EUS procedures carefully, requiring clear medical necessity before approving reimbursement. Understanding payer policies helps billing teams anticipate coverage requirements and address potential issues proactively. Common medically necessary indications include staging of esophageal or gastric malignancies, evaluation of submucosal lesions, and assessment of chronic pancreatitis complications.
Documentation must clearly link the EUS procedure to the patient's clinical presentation and explain why alternative diagnostic modalities proved insufficient. This becomes particularly important for high-cost procedures where payers may request additional justification or peer review.
Billing Strategies and Reimbursement Optimization
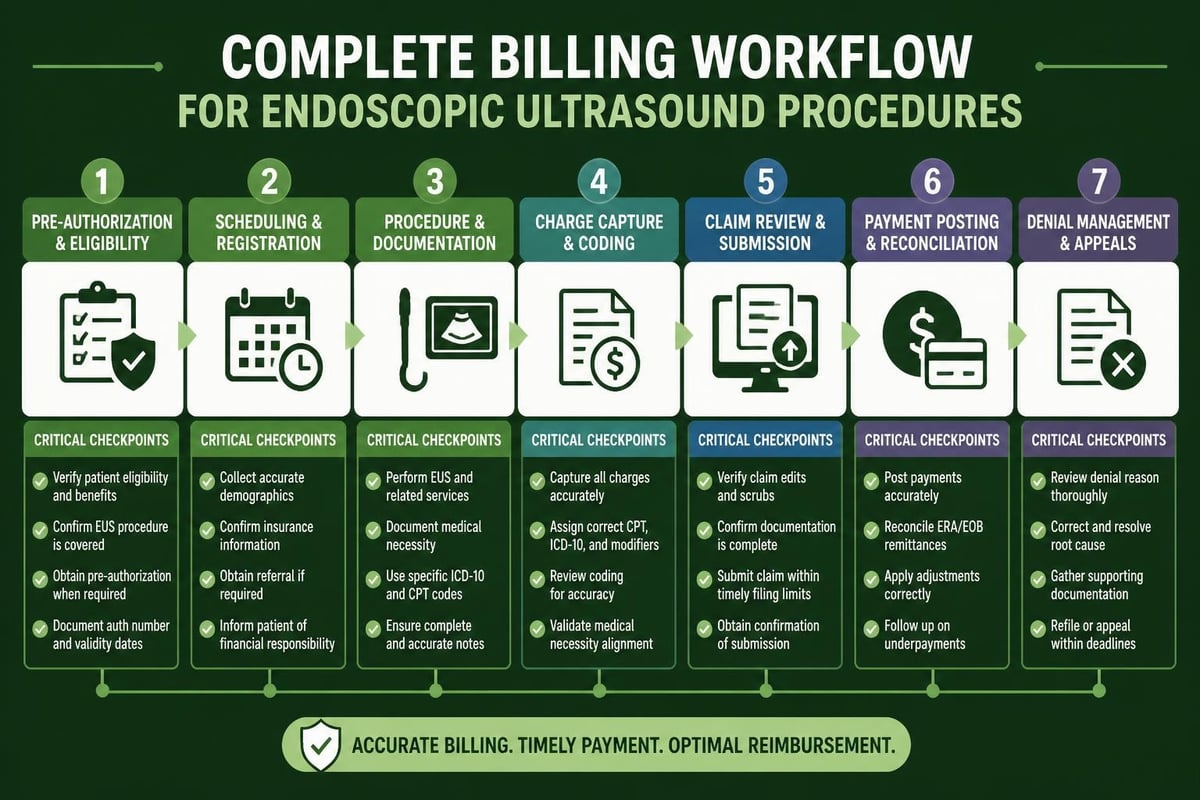
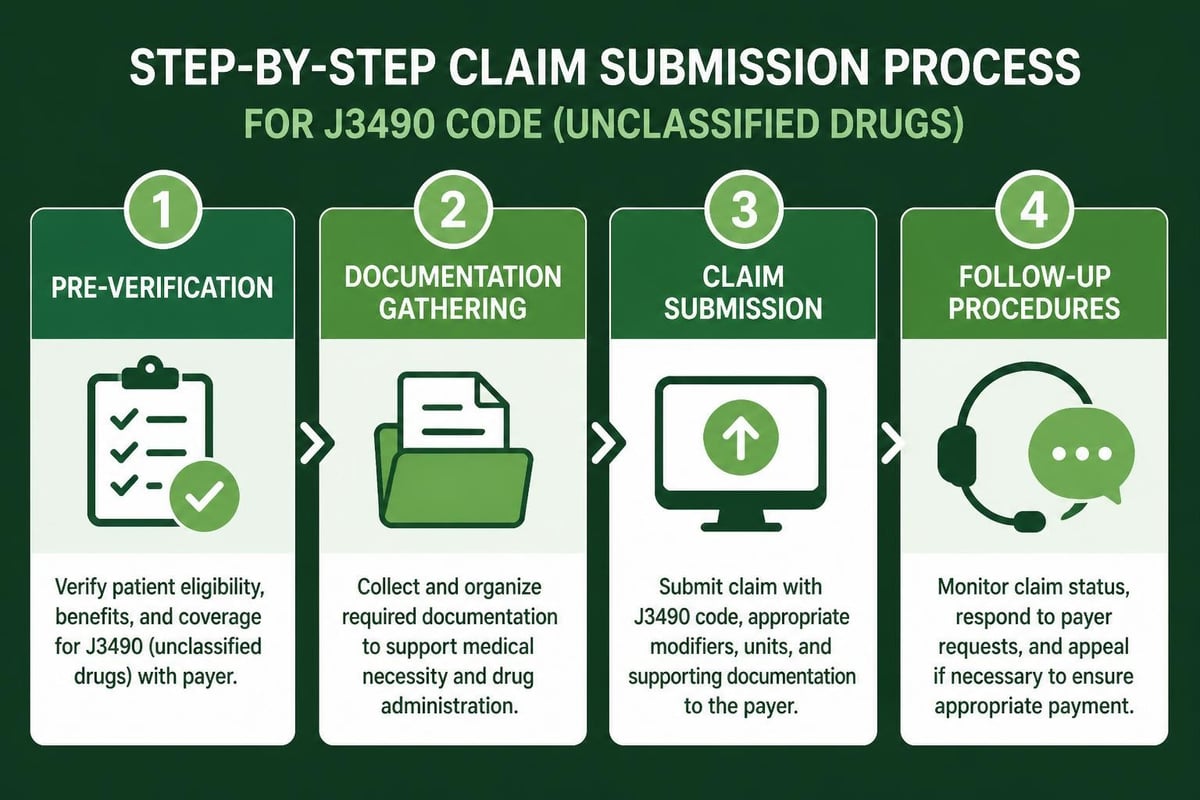
Successful EUS billing requires coordinated efforts across multiple revenue cycle functions. Pre-authorization represents the first critical step, as many commercial payers and Medicare Advantage plans require advance approval for EUS procedures. Verification teams must confirm coverage policies and obtain necessary authorizations before scheduling.
Coding accuracy directly influences reimbursement rates and claim acceptance. Practices utilizing medical billing software for small businesses benefit from built-in coding edits and compliance checks that flag potential issues before claim submission. These systems help identify common coding errors such as:
- Incorrect modifier usage with multiple procedures
- Unbundling of included services
- Missing or invalid diagnosis code linkage
- Improper site-of-service coding
- Failure to report sedation separately when applicable
Moderate Sedation Billing
According to EUS coding guidelines, moderate sedation should be billed separately when provided and documented appropriately. Prior to certain code revisions, sedation was bundled into many endoscopic procedures, but current guidelines allow separate reporting under specific circumstances.
Providers must document sedation administration, including pre-procedure assessment, intra-procedure monitoring, and post-procedure recovery observation. Time-based elements and personnel involved must appear clearly in the medical record to support separate sedation billing.
Common Coding Errors and Prevention
Revenue cycle teams frequently encounter specific errors when processing EUS claims that lead to denials or underpayment. Understanding these patterns helps practices implement preventive measures and improve clean claim rates. The relationship between proper CPT code usage and successful claim adjudication cannot be overstated.
Bundling and Unbundling Issues
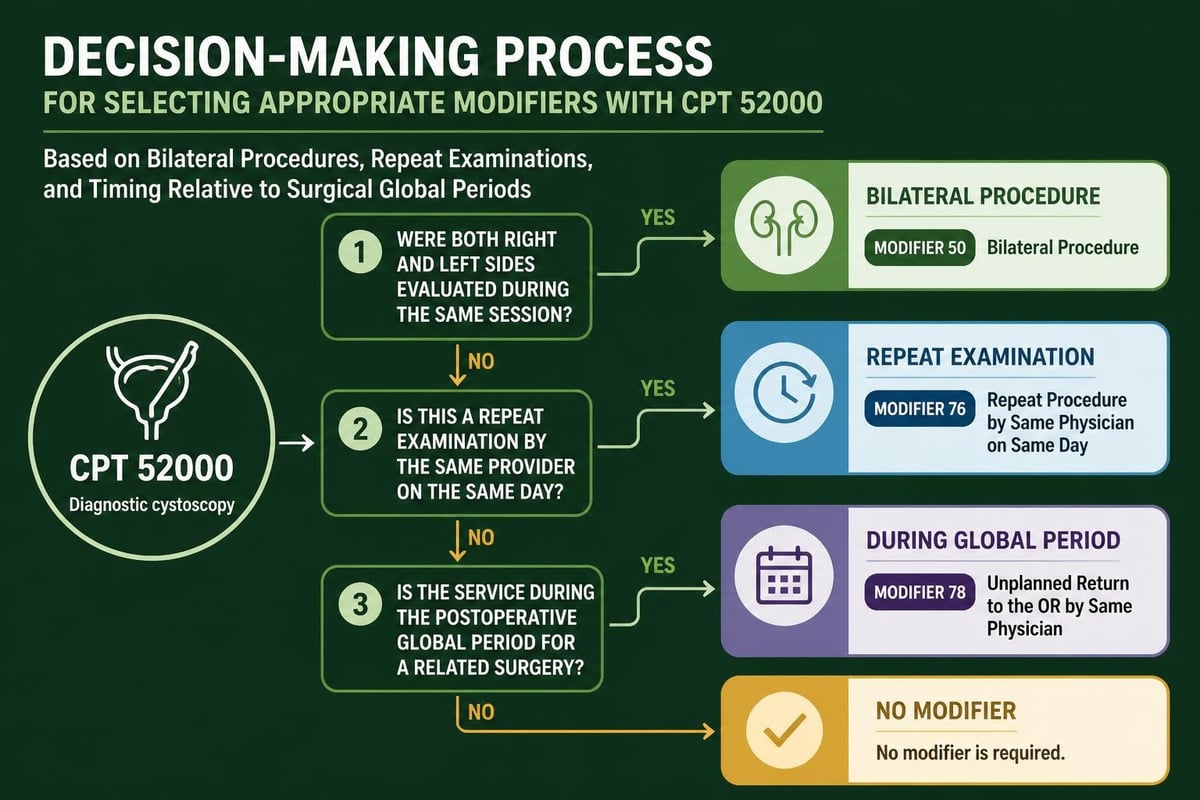
The National Correct Coding Initiative (NCCI) includes numerous edits affecting eus cpt code combinations. Billing teams must recognize which services bundle into the primary procedure and which qualify for separate reporting with appropriate modifiers. For example, biopsy obtained during diagnostic EUS typically requires a distinct code rather than being included in the base examination code.
Modifier application plays a crucial role in explaining code relationships and preventing inappropriate denials. Modifier 59 or its more specific X-modifiers may be necessary when reporting distinct procedural services performed during the same session.
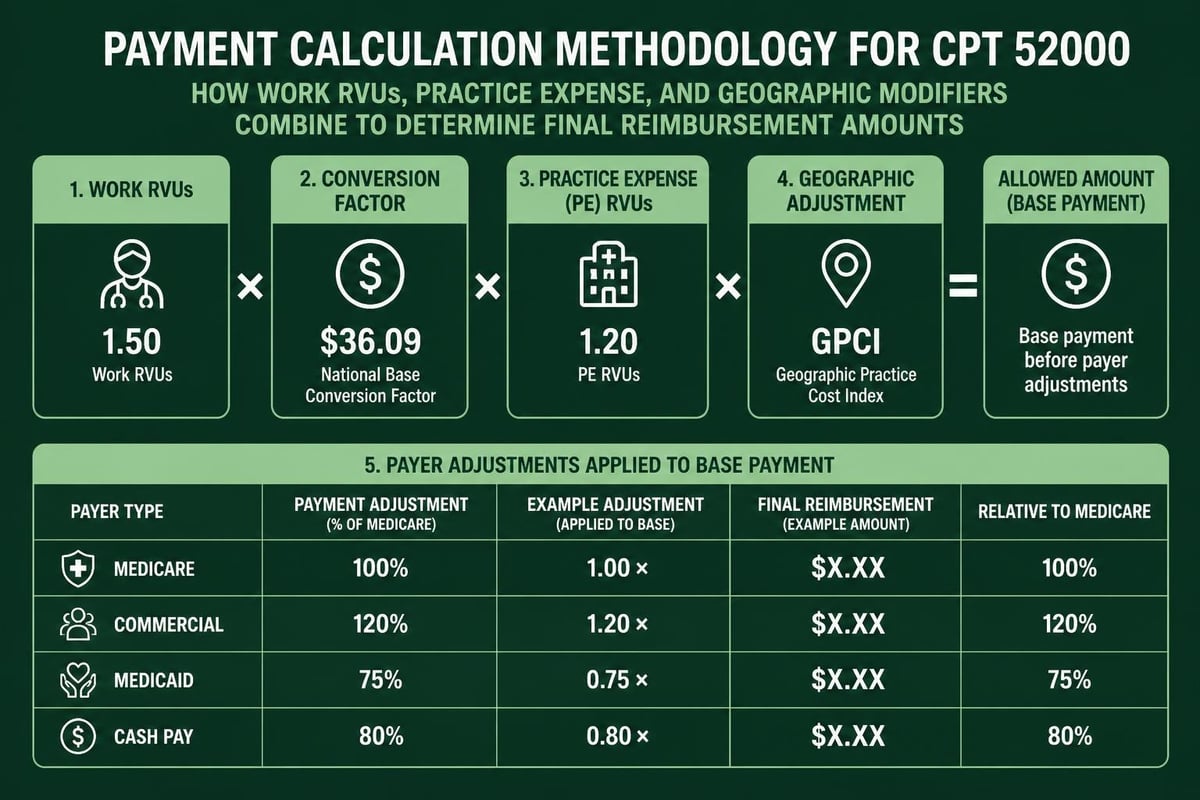
RVU Values and Payment Expectations
Understanding relative value units (RVUs) for EUS procedures helps practices forecast revenue and identify underpayment situations. CPT 43242 RVU data shows the work, practice expense, and malpractice components that determine Medicare payment rates. Commercial payers typically base their fee schedules on Medicare values with varying conversion factors.
Practices should regularly analyze payment patterns to identify payers consistently reimbursing below expected rates. This analysis supports contract negotiations and helps justify requests for improved fee schedules. Healthcare revenue cycle analytics provide the data foundation for these strategic discussions.
Payer-Specific Requirements
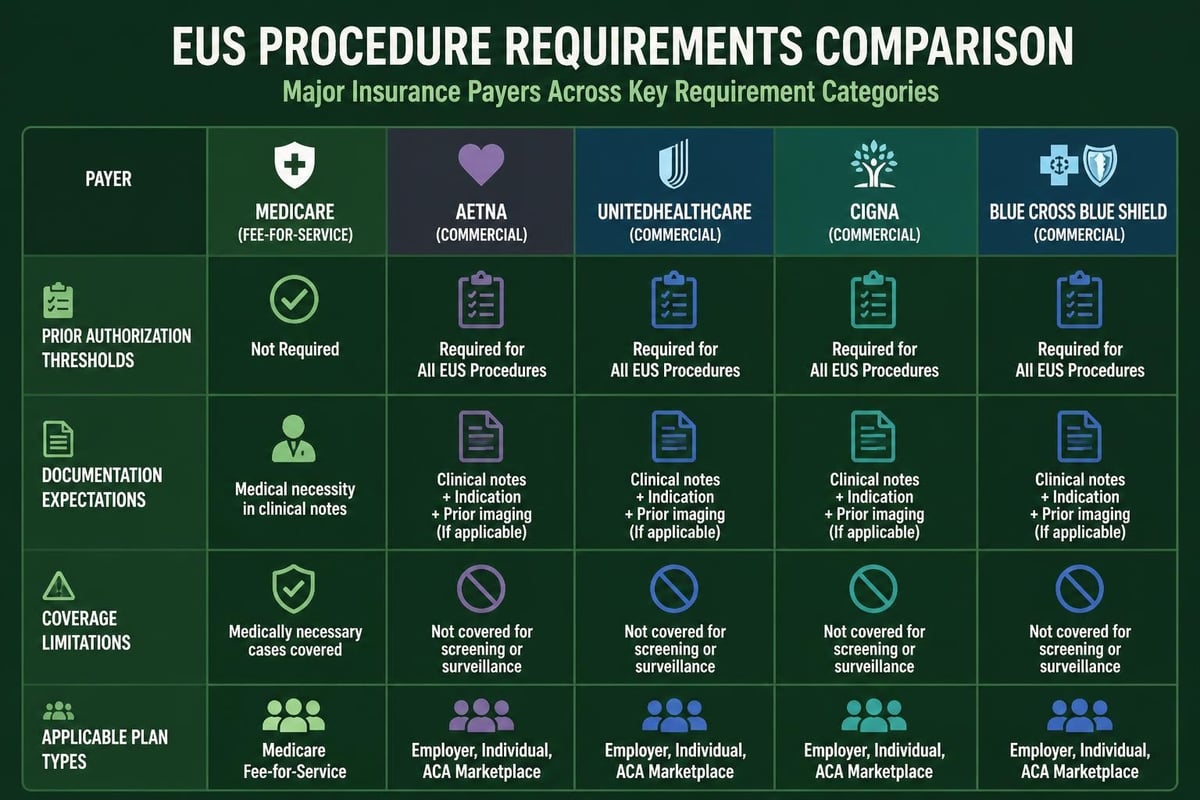
Different insurance carriers maintain varying policies regarding EUS coverage and billing requirements. Aetna’s clinical policy on endoscopic ultrasonography outlines medical necessity criteria and applicable CPT codes, demonstrating how payers establish coverage parameters. Billing specialists must familiarize themselves with major payer policies to ensure compliant claim submission.
Medicare coverage policies may differ from commercial payer requirements, particularly regarding local coverage determinations (LCDs) that apply in specific geographic regions. Practices serving diverse patient populations must track requirements across multiple payer contracts.
Appeals and Denial Management
When EUS claims face denial, systematic appeal processes become essential for revenue recovery. Effective denial management requires rapid response times and thorough documentation review to identify correctable errors versus legitimate payment refusals.
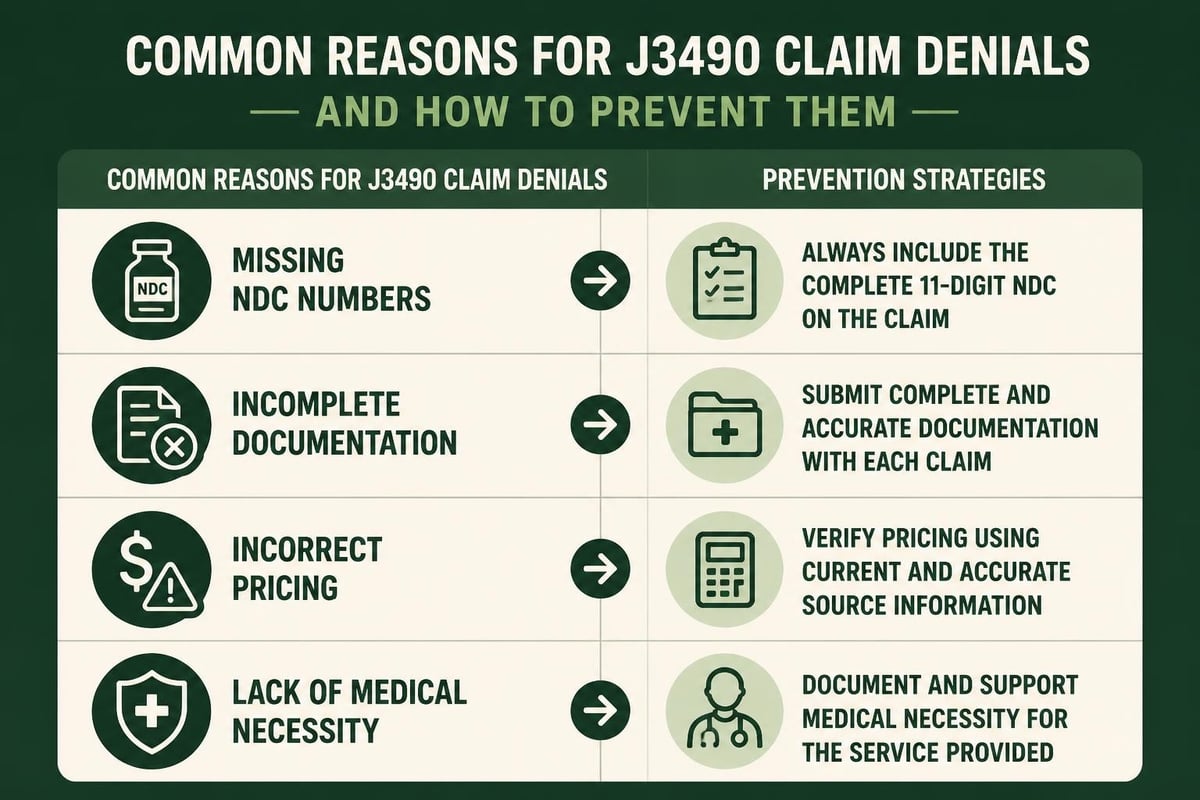
Common denial reasons include:
- Lack of medical necessity documentation
- Missing or invalid prior authorization
- Incorrect code selection for documented procedure
- Insufficient anatomical detail in procedure notes
- Failure to meet payer-specific coverage criteria
Appeal letters should directly address the specific denial reason with supporting clinical documentation and payer policy citations demonstrating coverage applicability. Many practices benefit from partnering with revenue cycle management specialists who understand gastroenterology-specific coding requirements and payer policies.
Compliance and Audit Preparedness
Regular internal audits of EUS coding practices help identify potential compliance risks before external auditors raise concerns. Practices should review samples of EUS procedures quarterly, comparing documentation against billed codes to ensure accuracy and completeness. This proactive approach protects against future audit liability and improves overall coding quality.
Billing and coding specialists with gastroenterology expertise provide valuable oversight for complex procedural coding like EUS services. Their specialized knowledge helps navigate the nuanced differences between similar codes and ensures documentation meets evolving payer standards.
Training programs should address updates to eus cpt code definitions, bundling edits, and coverage policies as they occur throughout the year. Continuous education maintains coding accuracy despite frequent regulatory changes affecting endoscopic procedures.
Accurate EUS CPT code selection and billing requires specialized knowledge of procedural variations, documentation standards, and payer requirements that directly impact practice revenue. Healthcare providers benefit significantly from partnering with experienced revenue cycle management professionals who understand these complexities and implement proven strategies for optimal reimbursement. Greenhive Billing Solutions delivers comprehensive medical billing services specifically designed for gastroenterology and specialty practices, ensuring accurate coding, timely claim submission, and effective denial management that maximizes your practice's financial performance while maintaining full compliance with regulatory requirements.