Understanding and managing claim denials represents one of the most significant challenges facing healthcare providers today. With denial rates averaging between 5% and 10% across the industry, mastering the most common denial codes in medical billing becomes essential for maintaining healthy cash flow and operational efficiency. Each denial code tells a specific story about what went wrong during the claim submission process, from simple administrative errors to complex coverage issues. By recognizing these patterns and implementing targeted prevention strategies, healthcare organizations can significantly reduce revenue loss and administrative burden while improving overall financial performance.
Understanding Medical Billing Denial Codes
Medical billing denial codes serve as standardized communication tools between payers and providers. These alphanumeric identifiers explain exactly why an insurance company rejected or denied a claim for payment. The Centers for Medicare & Medicaid Services (CMS) and various commercial payers use these codes to categorize denials into specific groups, making it easier for billing departments to identify trends and implement corrective actions.
Denial codes typically fall into several broad categories. Administrative denials stem from paperwork errors, missing information, or submission mistakes. Clinical denials involve medical necessity questions or lack of supporting documentation. Coverage denials occur when services fall outside the patient's benefit plan or policy limitations. Understanding these categories helps revenue cycle teams prioritize their denial management efforts and allocate resources effectively.
The financial impact of denials extends beyond the initial claim rejection. Each denied claim requires staff time to research, correct, and resubmit, creating a cascading effect on operational costs. According to industry research on common denial codes, practices spend an average of $25 to $30 in labor costs per reworked claim. This makes preventing denials far more cost-effective than managing them after the fact.
CO-16: Claim Lacks Information or Contains Formatting Errors
CO-16 represents one of the most frequently encountered denial codes across all specialties and payer types. This code indicates that the submitted claim lacks necessary information or contains formatting errors that prevent proper processing. The versatility of this code means it can apply to dozens of different scenarios, from missing National Provider Identifier (NPI) numbers to incorrect date formats.
Common triggers for CO-16 denials include:
- Missing or invalid patient demographic information
- Incorrect provider identifiers or taxonomy codes
- Improperly formatted procedure or diagnosis codes
- Absent or incomplete referring physician information
- Missing required attachments or supporting documentation
Prevention strategies focus on implementing robust front-end quality checks. Staff should verify all required fields are completed before claim submission, utilize clearinghouse scrubbing tools to catch formatting errors, and maintain updated provider enrollment information across all payers. Regular audits of denied claims coded as CO-16 help identify recurring patterns that point to specific workflow gaps.
Many practices benefit from standardized data entry protocols that ensure consistency across all claims. Creating detailed checklists for different claim types and specialty services reduces the likelihood of missing critical information. Professional denial management services can also implement systematic quality review processes that catch these errors before claims reach payers.
CO-22: Coordination of Benefits Issues
The CO-22 denial code signals problems with coordination of benefits (COB) when a patient has multiple insurance policies. Payers use this code when claims are submitted to the wrong insurance company or when the correct billing sequence isn't followed. This commonly affects Medicare beneficiaries with supplemental coverage, patients with employer-sponsored plans plus spouse coverage, and children covered under both parents' policies.
Resolving CO-22 Denials
Step 1: Verify the patient's current insurance coverage hierarchy through eligibility verification.
Step 2: Identify the primary payer based on coordination of benefits rules (birthday rule, Medicare Secondary Payer guidelines, etc.).
Step 3: Resubmit the claim to the correct primary insurance first.
Step 4: Bill the secondary payer only after receiving the primary payer's explanation of benefits.
Step 5: Update patient insurance information in your practice management system to prevent future errors.
Implementing comprehensive eligibility verification services at the point of scheduling and registration dramatically reduces CO-22 denials. Real-time eligibility checks reveal multiple active policies and their coverage hierarchy, allowing staff to collect accurate information before services are rendered. This proactive approach prevents the time-consuming appeals process required after denial.
| CO-22 Prevention Tactic | Implementation Method | Expected Impact |
|---|---|---|
| Real-time eligibility verification | Check benefits at scheduling and check-in | 70-80% reduction |
| Patient insurance questionnaire | Ask about all active policies during intake | 60-65% reduction |
| COB rules training | Educate staff on Medicare, birthday rule, etc. | 50-60% reduction |
| Automated alerts | Flag accounts with multiple active insurances | 75-85% reduction |
CO-27: Missing or Incomplete Service Facility Location
CO-27 denials occur when claims lack complete information about where services were provided. Payers require specific details about the service facility, including the facility name, address, and NPI number. This code appears frequently for procedures performed at locations other than the provider's primary office, such as hospital outpatient departments, ambulatory surgical centers, or skilled nursing facilities.
Different place of service (POS) codes require different levels of facility detail. For example, services billed with POS 22 codes must include complete hospital information. Similarly, procedures performed at ambulatory surgical centers need the facility's unique identifiers to process correctly.
Preventing CO-27 denials requires meticulous attention to documentation workflows. Create facility information databases that staff can easily reference when entering claims. Establish clear protocols for obtaining facility NPI numbers and addresses from hospital registration departments or ASC administrators. Train coding and billing staff to recognize which POS codes trigger facility information requirements.
PR-1: Deductible Amount
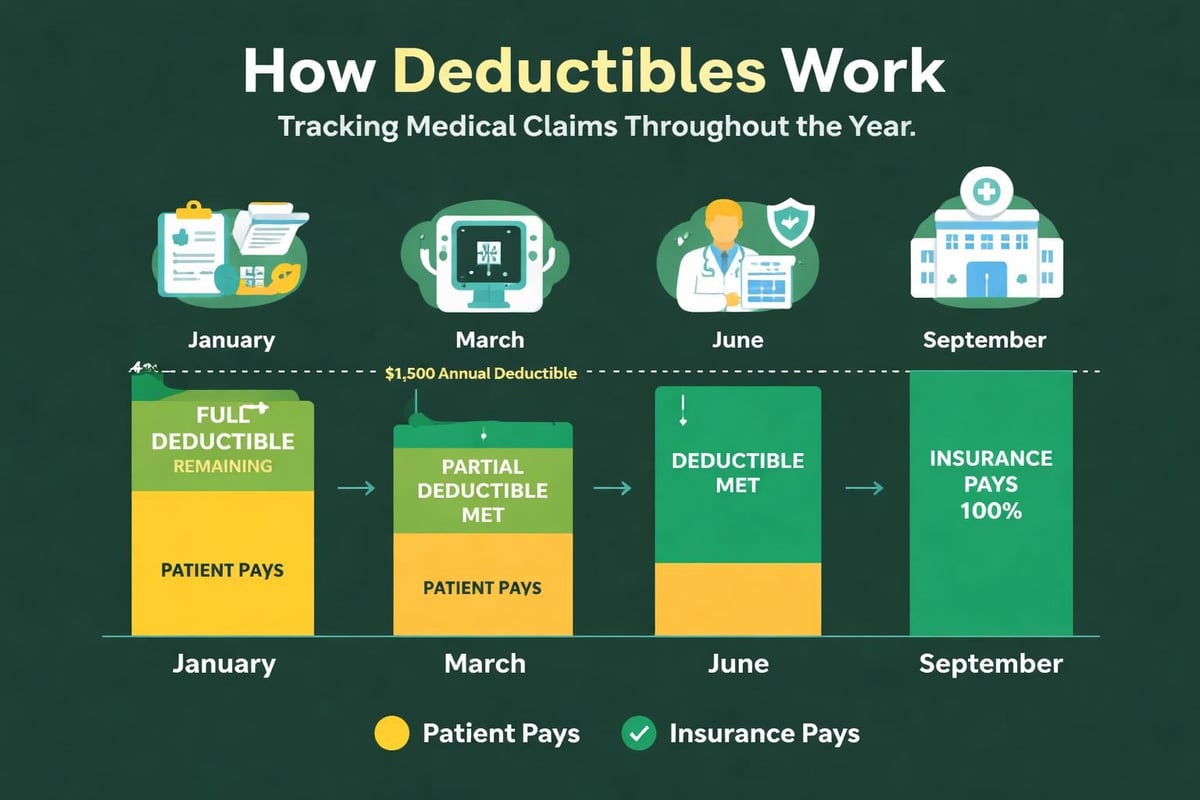
The PR-1 denial code indicates that the patient's insurance deductible hasn't been met, making the patient responsible for the charges. While technically not a true denial (the claim was processed correctly), this adjustment category creates collection challenges for many practices. Understanding how deductibles work and communicating these obligations clearly to patients prevents confusion and improves collection rates.
Deductible-related adjustments spike at the beginning of each calendar year when annual deductibles reset. Practices experience higher patient responsibility balances during January through March, requiring enhanced patient communication strategies during these months. High-deductible health plans (HDHPs) have amplified this challenge, as more patients carry individual deductibles of $1,500 to $7,000 or higher.
Effective strategies for managing PR-1 adjustments:
- Verify deductible status during eligibility checks and inform patients before services
- Collect estimated patient portions at time of service when possible
- Offer payment plans for patients facing large deductible amounts
- Send clear, itemized statements explaining deductible applications
- Train front desk staff to discuss financial responsibility compassionately
Many revenue cycle management companies implement sophisticated patient estimation tools that calculate expected out-of-pocket costs based on current deductible status. These estimates help patients plan financially and increase the likelihood of timely payment. Transparent communication about costs builds trust and reduces payment friction.
CO-50: Non-Covered Services
CO-50 denials indicate that the service provided isn't covered under the patient's insurance plan. This represents a contractual obligation issue rather than a claim error. Services might be excluded based on the specific policy type, considered experimental or investigational, or fall outside the scope of medically necessary care as defined by the payer.
Non-covered service denials present particular challenges because they often can't be appealed successfully unless documentation proves the service actually differs from what the payer believed was performed. Prevention becomes the primary strategy, requiring robust prior authorization services and patient communication protocols.
Healthcare providers should obtain advance beneficiary notices (ABNs) for Medicare patients when services may not be covered. For commercial payers, practices should verify coverage for specialized procedures, durable medical equipment, and newer treatments before rendering services. Clear documentation of these conversations protects the practice's ability to bill patients directly when services aren't covered.
CO-97: Payment Included in Allowance for Another Service
The CO-97 code appears when payers bundle services together under a single payment rather than reimbursing each component separately. This frequently affects surgical procedures with included postoperative care, diagnostic tests performed together, or services that fall under global payment methodologies. Understanding bundling rules and the National Correct Coding Initiative (NCCI) edits helps prevent these denials.
Common CO-97 Scenarios
Surgical global periods that include pre-operative visits, the procedure itself, and post-operative follow-up appointments typically generate CO-97 denials if providers bill these components separately. Laboratory panels that include multiple individual tests result in denials when each test is billed independently. E/M services performed on the same day as procedures may bundle into the procedure payment depending on the circumstances and appropriate modifier usage.
Preventing CO-97 denials requires comprehensive knowledge of:
- NCCI edits and their quarterly updates
- Payer-specific bundling policies that may differ from Medicare
- Appropriate modifier usage (modifier 25, 59, etc.) to indicate separately identifiable services
- Global surgical package definitions for different procedure types
- Component versus panel coding for laboratory and diagnostic services
Investing in regular training on coding services ensures staff stay current with evolving bundling rules. Many practices implement coding audit programs that review claims before submission, catching potential bundling issues that would result in CO-97 denials.
CO-4: Duplicate Claim Submission
CO-4 denials occur when payers receive what appears to be a duplicate claim for the same patient, date of service, and procedure codes. While some CO-4 denials represent genuine duplicate submissions resulting from system errors or miscommunication, others occur when providers legitimately performed the same service multiple times on different dates, but claim formatting makes them appear identical.
True duplicate submissions waste processing resources and delay legitimate reimbursement. They commonly result from inadequate claim tracking systems, communication breakdowns between departments, or attempts to expedite payment by resubmitting claims still in processing status. Establishing clear protocols for claim status checks and resubmissions prevents most genuine duplicate scenarios.
| Duplicate Prevention Strategy | Tool/Method | Effectiveness |
|---|---|---|
| Claim tracking system | Practice management software flags | Very High |
| Daily submission reports | Review batches before clearinghouse transmission | High |
| Payer portal checks | Verify claim status before resubmission | High |
| 30-day wait policy | Standard time before claim follow-up | Moderate |
When CO-4 denials represent situations where the same service was actually performed on different dates, detailed documentation and appeals become necessary. Medical claim submission services implement sophisticated tracking mechanisms that prevent duplicate submissions while ensuring legitimate claims reach payers promptly.
PR-96: Non-Covered Charges
The PR-96 code indicates patient responsibility for non-covered charges, similar to CO-50 but specifically transferring financial obligation to the patient. This commonly applies to cosmetic procedures, experimental treatments, services exceeding plan limitations, or care received from out-of-network providers under plans without out-of-network benefits.
Effective financial counseling prevents surprise bills and collection challenges associated with PR-96 adjustments. Practices should provide written estimates for elective procedures not typically covered by insurance, discuss out-of-network implications before scheduling appointments, and obtain written acknowledgment that patients understand their financial responsibility.
For services that might not be covered, thorough documentation of medical necessity becomes critical. While PR-96 indicates the patient owes the balance, appropriate documentation and appeals can sometimes shift responsibility back to the payer if coverage determinations were incorrect. This particularly applies when denials stem from insufficient documentation rather than genuine coverage exclusions.
CO-109: Claim Not Covered by This Payer
CO-109 appears when claims are submitted to the wrong insurance company or when patients' coverage has terminated. This code essentially says "we're not responsible for paying this claim." Common causes include outdated insurance information, patients switching employers or plans, coverage lapses due to non-payment of premiums, or incorrect coordination of benefits information.
Reducing CO-109 denials centers on rigorous eligibility verification processes. Checking insurance eligibility at multiple touchpoints-when appointments are scheduled, 24-48 hours before the appointment, and again at check-in-catches most coverage changes before services are rendered. Real-time eligibility systems integrate directly with practice management platforms, automatically flagging coverage issues that require patient contact.
When CO-109 denials occur despite verification efforts, prompt patient communication becomes essential. Contact patients immediately to obtain current insurance information, reverify eligibility with the correct payer, and resubmit claims within timely filing limits. Many payers allow only 90-180 days from the date of service for initial claim submission, making quick action critical.
CO-18: Exact Duplicate Claim
While similar to CO-4, the CO-18 code specifically identifies exact duplicate claims where every data element matches a previously submitted claim. This more definitive duplicate designation indicates the payer's system has already received and processed (or is processing) an identical claim. Unlike situations where dates or other elements differ slightly, CO-18 represents clear redundancy.
Prevention strategies for CO-18 denials include implementing clearinghouse validations that check for duplicates before transmission, maintaining comprehensive claim submission logs with batch numbers and transmission dates, and establishing clear communication channels between staff members who might independently attempt to submit the same claim.
Most practice management systems and billing platforms offer built-in duplicate detection features. However, these tools only work if staff members understand and utilize them correctly. Regular training on billing software systems ensures team members leverage available technology to prevent avoidable errors.
CO-29: Time Limit for Filing Expired
The CO-29 denial code represents missed filing deadlines, one of the most financially damaging denial types because these claims typically can't be appealed or resubmitted. Each payer establishes specific timeframes within which they'll accept claims, ranging from 90 days to one year from the date of service. Missing these deadlines results in permanent revenue loss.
Timely filing denials often stem from delays earlier in the revenue cycle process. Common causes include:
- Slow charge entry from providers or clinics
- Extended appeals processes on initially denied claims
- Waiting for patients to provide current insurance information
- Internal workflow bottlenecks in coding or billing departments
- System downtimes or technical issues preventing claim transmission
Preventing CO-29 denials requires systematic workflows that move claims through each revenue cycle stage efficiently. Establish internal deadlines well before actual payer filing limits, implement automated alerts for claims approaching deadlines, track aging reports daily to identify bottlenecks, and prioritize older claims in work queues.
Timely Filing Deadlines by Common Payer Type:
| Payer Type | Typical Filing Deadline | Notes |
|---|---|---|
| Medicare | 1 year from date of service | Calendar year or rolling 12 months |
| Medicaid | 90-180 days (state-specific) | Varies significantly by state |
| Commercial plans | 90-365 days | Review each contract |
| Workers' compensation | 90-120 days | State-regulated |
| Auto insurance | 30-90 days | Policy-dependent |
Professional revenue cycle management teams track these deadlines meticulously and maintain organized workflows that ensure claims are submitted with adequate time for payer processing and potential resubmission if initial attempts fail. Understanding how denial management improves cash flow helps practices appreciate the critical importance of timely filing compliance.
Patterns in the Most Common Denial Codes
Analyzing patterns across the most common denial codes in medical billing reveals systemic issues that practices can address through targeted interventions. Many denials cluster around specific failure points in the revenue cycle, suggesting opportunities for process improvement that yield significant financial returns.
Front-end revenue cycle processes account for approximately 60-70% of denial causes. Insurance verification failures, incomplete demographic information, missing referrals and authorizations, and inadequate patient financial counseling all contribute to downstream denials. Strengthening intake procedures and eligibility verification protocols prevents numerous CO-16, CO-22, CO-109, and PR-1 issues.
Coding accuracy impacts another 20-30% of denials. Understanding different types of medical coding and maintaining current knowledge of code updates, bundling rules, and modifier requirements reduces CO-97, CO-50, and similar clinical denials. Regular medical coding audits identify education opportunities and compliance risks before they generate widespread denials.
Billing and submission processes contribute the remaining 10-20% of common denials. CO-4, CO-18, and CO-29 denials typically stem from workflow issues, technology gaps, or inadequate claim tracking rather than clinical or administrative errors. Implementing robust claim scrubbing, status tracking, and deadline management systems addresses these operational challenges.
Building a Proactive Denial Prevention Program
Shifting from reactive denial management to proactive denial prevention requires commitment and structured implementation. Healthcare organizations that successfully reduce denial rates typically follow a systematic approach that addresses root causes rather than simply working denials after they occur.
Key components of effective denial prevention:
- Data analytics: Track denial rates by code, payer, provider, and service type to identify patterns
- Root cause analysis: Investigate why denials occur rather than just correcting individual claims
- Staff education: Provide ongoing training on coding updates, payer policy changes, and best practices
- Technology optimization: Leverage clearinghouse edits, eligibility systems, and workflow automation
- Performance monitoring: Establish metrics and dashboards that make denial trends visible
- Continuous improvement: Implement regular review cycles that refine processes based on results
Many practices partner with specialized revenue cycle management providers who bring expertise, dedicated resources, and proven methodologies for reducing denials. These partnerships allow healthcare providers to focus on clinical care while ensuring their revenue cycle operates at peak efficiency.
According to research on claim denial management, organizations that implement comprehensive denial prevention programs typically reduce their denial rates by 30-50% within the first year. This translates to significant revenue recovery and reduced administrative burden across the billing department.
Technology's Role in Managing Denial Codes
Modern revenue cycle technology offers powerful tools for identifying, preventing, and resolving the most common denial codes in medical billing. Advanced clearinghouse systems perform hundreds of validation checks before claims reach payers, catching formatting errors, missing information, and coding issues that trigger CO-16 and similar denials.
Artificial intelligence and machine learning algorithms now analyze historical denial patterns to predict which claims carry high denial risk. These predictive analytics tools flag problematic claims for manual review before submission, preventing denials rather than merely managing them afterward. Some systems even suggest specific corrections based on past successful resolutions of similar issues.
Integration between eligibility verification systems, practice management platforms, and billing software creates seamless workflows that reduce manual data entry and the errors it introduces. Real-time eligibility checks prevent CO-22 and CO-109 denials by ensuring current insurance information flows automatically through each system touchpoint.
Automated workflow tools also help manage the most common denial codes by routing different denial types to appropriate team members based on specialization. Claims denied for CO-16 issues route to data entry specialists for correction, while CO-50 denials requiring clinical documentation route to coding staff or providers. This specialization improves resolution efficiency and reduces turnaround time.
Many healthcare organizations use comprehensive reporting and analytics platforms that provide visibility into denial trends, allowing leadership to make data-driven decisions about resource allocation and process improvements. These insights help practices prioritize which denial types offer the greatest opportunity for revenue recovery and prevention.
Staff Training and Denial Code Expertise
Even the best technology requires knowledgeable users who understand denial codes and their implications. Building team expertise around the most common denial codes in medical billing creates a culture of quality that prevents errors throughout the revenue cycle. Different staff members need varying levels of knowledge based on their roles.
Front desk and registration staff should understand how incomplete or inaccurate information collected during intake creates downstream denials. Training these team members on CO-16, CO-22, and CO-109 prevention helps them appreciate how their work directly impacts practice revenue. They don't need to understand complex coding rules, but they must recognize the importance of complete demographic and insurance information.
Coding professionals require deep knowledge of clinical denial codes like CO-50 and CO-97. Understanding medical necessity guidelines, bundling rules, and appropriate modifier usage prevents denials before claims are submitted. Ongoing education on code updates and payer policy changes keeps coding staff current with evolving requirements.
Billing specialists need comprehensive knowledge across all denial categories since they manage claims after submission. They must understand payer-specific variations in how common codes are applied, appeal strategies for different denial types, and timely filing requirements that govern resubmission opportunities. This broad expertise allows them to triage denials effectively and pursue the most appropriate resolution path.
Regular case studies using actual denials from the practice provide practical learning opportunities. Reviewing common billing and coding errors that occurred within the organization makes training relevant and demonstrates real financial impact. This approach builds engagement and reinforces the connection between individual actions and practice financial health.
Measuring Success in Denial Management
Establishing clear metrics for tracking denial performance helps organizations assess whether prevention strategies are working. The most meaningful key performance indicators (KPIs) examine both denial frequency and resolution effectiveness, providing a comprehensive view of revenue cycle health.
Primary denial management metrics include:
| Metric | Formula | Target Benchmark |
|---|---|---|
| Initial denial rate | Denied claims / Total claims submitted | Less than 5% |
| Denial write-off rate | Denied dollars not recovered / Total denied dollars | Less than 2% |
| Days in A/R (denied) | Average days to resolve denied claims | Less than 30 days |
| Clean claim rate | Claims paid on first submission / Total claims | Greater than 95% |
| Denial overturn rate | Successfully appealed denials / Total appeals | Greater than 60% |
Tracking these metrics by denial code type reveals which areas require focused attention. A practice might have excellent overall denial rates but struggle specifically with CO-97 bundling issues or CO-29 timely filing problems. Drilling down into denial code-specific performance enables targeted interventions rather than broad, unfocused improvement efforts.
Benchmarking against industry standards and similar practices provides context for performance evaluation. Resources like comprehensive analysis of denial trends help organizations understand whether their denial rates reflect typical challenges or indicate areas requiring immediate attention.
Regular reporting cycles-weekly for operational metrics, monthly for trending analysis, and quarterly for strategic review-keep denial management visible to leadership and maintain organizational focus on continuous improvement. Dashboard tools that visualize these metrics make complex data accessible to stakeholders at all levels.
Mastering the most common denial codes in medical billing transforms revenue cycle performance by preventing lost revenue and reducing administrative burden. By implementing systematic prevention strategies, leveraging technology effectively, and building team expertise, healthcare organizations can achieve dramatic improvements in clean claim rates and days to payment. Greenhive Billing Solutions partners with healthcare providers nationwide to implement comprehensive denial management programs that identify root causes, prevent common denials, and recover maximum revenue. Our experienced team brings proven methodologies and dedicated resources that allow practices to focus on patient care while ensuring financial sustainability.

