Medical coding serves as the backbone of revenue cycle management, transforming clinical documentation into standardized codes that drive reimbursement for healthcare providers. The integration of rcm medical coding processes directly impacts cash flow, compliance, and overall financial health of medical practices. Understanding how coding functions within the broader revenue cycle enables healthcare organizations to optimize their billing operations, reduce claim denials, and accelerate payment collection. This comprehensive guide explores the critical role coding plays in RCM, the challenges providers face, and strategies to enhance coding accuracy for improved financial outcomes.
The Foundation of RCM Medical Coding
RCM medical coding represents the systematic process of translating medical services, diagnoses, procedures, and equipment into universal alphanumeric codes. These standardized codes form the language between healthcare providers and payers, ensuring accurate communication about services rendered. The AAPC provides detailed information on medical coding certifications and standards that professionals must follow to maintain compliance.
Three primary code sets dominate the medical coding landscape. ICD-10-CM codes classify diagnoses and medical conditions, containing over 70,000 codes that describe patient health status. CPT codes define medical procedures and services performed by healthcare professionals, covering everything from routine office visits to complex surgical interventions. HCPCS Level II codes identify products, supplies, and services not included in CPT codes, such as durable medical equipment and ambulance services.
The accuracy of these codes determines reimbursement levels and claim acceptance rates. When coders properly match diagnosis codes with procedure codes, they establish medical necessity and justify the services provided. This documentation integrity forms the foundation of successful revenue cycle operations.
Integration Points Within Revenue Cycle Management
Medical coding intersects with virtually every stage of the revenue cycle, creating dependencies that affect overall performance. The coding phase occurs after clinical documentation but before claims submission, making it a critical control point for revenue capture.
Key integration points include:
- Patient registration and eligibility verification systems that inform coding requirements
- Charge capture processes that identify all billable services
- Claims submission platforms that validate code combinations
- Payment posting systems that reconcile expected versus actual reimbursement
- Denial management workflows that address coding-related rejections
Understanding different types of medical coding helps providers appreciate how various coding specialties support different practice types and service lines. Specialty-specific coding knowledge becomes essential for practices offering complex services or treating specific patient populations.
Critical Components of Effective RCM Medical Coding
Successful rcm medical coding operations require multiple components working in harmony. Each element contributes to accuracy, efficiency, and compliance, ultimately affecting the bottom line for healthcare providers.
Documentation Quality and Specificity
Clinical documentation provides the source material for accurate coding. Without detailed, specific documentation from providers, coders cannot assign the most appropriate codes that reflect the complexity and medical necessity of services rendered. The CMS guidance on fee-for-service claims processing emphasizes the importance of documentation quality in supporting proper coding.
Providers must document the level of service, medical decision-making complexity, time spent, and specific details about diagnoses and procedures. Incomplete or vague documentation forces coders to query providers, delaying claim submission and payment. Many practices implement clinical documentation improvement programs to train providers on documentation requirements that support optimal coding.
Documentation best practices include:
- Recording specific anatomical locations for procedures and diagnoses
- Documenting all chronic conditions that affect patient care during each encounter
- Noting complications, comorbidities, and severity indicators
- Capturing time-based elements for evaluation and management services
- Linking procedures to supporting diagnoses that establish medical necessity
When documentation meets coding requirements without extensive queries, the revenue cycle moves more smoothly from service delivery to reimbursement.
Code Assignment Accuracy and Compliance
Accurate code assignment demands extensive knowledge of coding guidelines, payer policies, and clinical terminology. Professional coders must stay current with annual code updates, quarterly revisions, and payer-specific requirements that affect code selection. The Centers for Medicare & Medicaid Services offers official resources on ICD-10 coding that coders reference regularly to maintain compliance.
Coders analyze clinical documentation, apply official coding guidelines, and select codes that most accurately represent the services provided. This process requires clinical knowledge to understand medical terminology, procedures, and diagnoses, combined with coding expertise to navigate complex classification systems.
| Coding Accuracy Factor | Impact on RCM | Risk of Inaccuracy |
|---|---|---|
| Specificity | Higher reimbursement for detailed codes | Downcoding and lost revenue |
| Medical Necessity | Claim acceptance by payers | Denials and payment delays |
| Modifier Usage | Correct payment for unusual circumstances | Claim rejections or underpayment |
| Bundling Rules | Appropriate separate payments | Compliance issues and audits |
Coding errors create downstream problems throughout the revenue cycle. Undercoding leaves money on the table by failing to capture the full scope of services. Overcoding creates compliance risks and potential fraud allegations. Incorrect code combinations trigger automated claim rejections, requiring rework and delaying payment.
Technology and Automation in Coding Operations
Modern rcm medical coding increasingly leverages technology to improve accuracy and efficiency. Computer-assisted coding systems analyze clinical documentation and suggest appropriate codes, helping coders work faster while maintaining quality. These systems cross-reference documentation against coding databases and apply logic rules to identify the most likely code choices.
Automated coding works best for straightforward encounters with clear documentation. Complex cases still require human expertise to interpret nuanced clinical situations and apply appropriate codes. The optimal approach combines technology with skilled coders who validate automated suggestions and handle exceptions.
Technology contributions to coding operations:
- Real-time code validation checking for compliance with payer edits
- Natural language processing extracting codeable information from clinical notes
- Encoder software providing coding guidance and references
- Scrubbing tools identifying potential errors before claim submission
- Analytics dashboards tracking coding productivity and accuracy metrics
Understanding what billing and coding specialists do clarifies how human expertise complements technological tools in delivering accurate coding results. The combination of skilled professionals and advanced systems produces the best outcomes for revenue cycle performance.
Revenue Impact of Medical Coding Excellence
The quality of medical coding directly correlates with financial performance across multiple revenue cycle metrics. Organizations that invest in coding excellence see measurable improvements in days in accounts receivable, clean claim rates, and net collection ratios.
First-Pass Resolution and Clean Claims
Clean claims that pass payer edits on first submission accelerate cash flow and reduce administrative costs. Medical coding accuracy represents the primary factor determining whether claims clear initial validation without rejections or requests for additional information. The HFMA provides insights into revenue cycle management best practices that emphasize clean claim optimization.
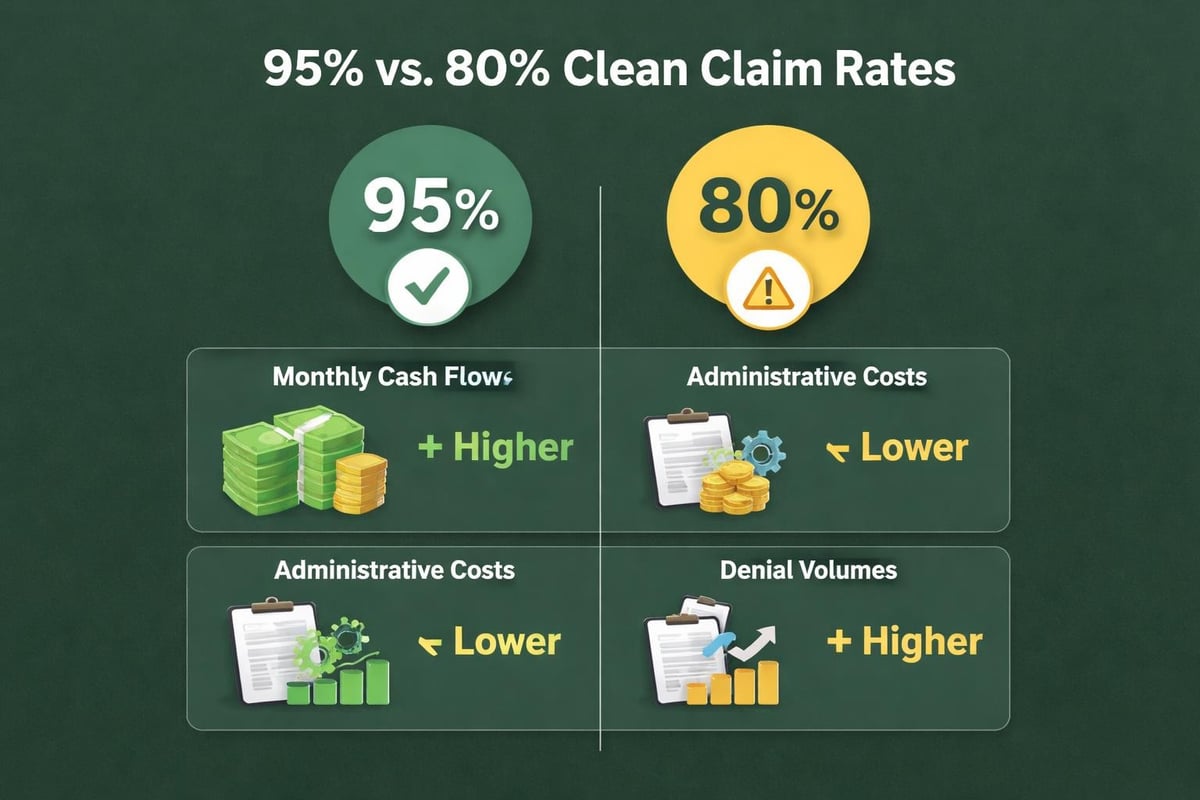
Industry benchmarks suggest top-performing organizations achieve clean claim rates above 95%, while average performers struggle with rates between 75% and 85%. The difference of 10 to 20 percentage points in clean claim rates translates to significant variations in payment speed and administrative burden.
Consider a practice submitting 5,000 claims monthly with an 80% clean claim rate versus 95%. The lower-performing practice must rework 1,000 claims monthly, requiring staff time, delaying payment, and risking reduced reimbursement. The higher-performing practice reworks only 250 claims, freeing staff for other revenue cycle activities.
Medical coding excellence drives clean claim rates through:
- Proper code selection that matches payer coverage policies
- Appropriate modifier usage that explains unusual circumstances
- Correct code sequencing following payer-specific requirements
- Valid code combinations that pass automated edits
- Supporting documentation that establishes medical necessity
Organizations focusing on these fundamentals consistently outperform competitors in first-pass resolution rates and collection speed.
Denial Prevention and Revenue Preservation
Coding-related denials represent one of the largest sources of preventable revenue loss in healthcare. Common coding denials include medical necessity failures, invalid code combinations, missing or incorrect modifiers, and lack of specificity. Understanding how denial management improves cash flow helps providers appreciate the connection between coding accuracy and revenue preservation.
Each denied claim creates additional work for billing staff who must research the denial reason, determine the appropriate response, and resubmit or appeal the claim. This rework costs between $25 and $117 per claim depending on complexity, according to industry research. Beyond direct costs, denied claims delay payment and risk eventual write-offs if appeal deadlines pass.
| Denial Category | Primary Coding Causes | Prevention Strategies |
|---|---|---|
| Medical Necessity | Diagnosis doesn't support procedure | Improved documentation linking clinical rationale |
| Invalid Codes | Deleted or incorrect code assignments | Regular updates to coding databases |
| Bundling Edits | Inappropriate unbundling of services | CCI edit checking before submission |
| Missing Information | Incomplete modifier or diagnosis data | Pre-submission claim scrubbing |
Proactive denial prevention through coding accuracy costs far less than reactive denial management. Organizations that invest in coder training, technology tools, and quality assurance processes see denial rates drop by 30% to 50% within the first year.
Compliance and Audit Readiness
Accurate rcm medical coding protects organizations from compliance risks and audit findings that threaten revenue and reputation. Government audits, payer reviews, and compliance investigations scrutinize coding patterns looking for evidence of fraud, abuse, or systematic errors. Proper coding practices demonstrate good faith efforts to bill correctly and maintain compliance with regulations.
Auditors examine multiple aspects of coding operations during reviews. They verify that codes match documented services, check for appropriate modifier usage, validate medical necessity linkages, and assess overall coding patterns for statistical outliers. Organizations with strong coding programs and documented quality assurance processes fare better during audits than those with ad hoc approaches.
Audit preparation through coding excellence includes:
- Regular internal audits sampling coded encounters for accuracy
- Documentation of coder training and certification maintenance
- Written coding policies reflecting current guidelines and payer requirements
- Query processes ensuring complete documentation before coding
- Monitoring systems tracking coding productivity and accuracy trends
When audits occur, organizations with robust coding programs can demonstrate their commitment to accuracy and compliance. This documentation often results in reduced extrapolation of audit findings and lower repayment demands. Knowledge of revenue coding principles helps organizations maintain compliant coding across inpatient and outpatient settings.
Overcoming Common RCM Medical Coding Challenges
Healthcare organizations face persistent challenges in maintaining coding quality while managing costs and meeting productivity demands. Addressing these obstacles requires strategic approaches that balance accuracy, efficiency, and resource constraints.
Coder Recruitment and Retention
The shortage of qualified medical coders creates recruitment challenges for healthcare organizations nationwide. Certified coders with specialty experience command premium salaries, and competition for talent remains intense. High turnover rates disrupt coding operations, requiring constant training and creating quality inconsistencies.
Many organizations partner with specialized RCM service providers to access experienced coding talent without the challenges of direct recruitment and retention. These partnerships provide flexibility to scale coding resources based on volume fluctuations while maintaining consistent quality through established training programs and quality assurance processes.
Service providers bring several advantages to coding operations:
- Immediate access to certified coders without recruitment delays
- Backup coverage preventing bottlenecks during staff absences
- Specialty coding expertise for complex service lines
- Established training programs maintaining current knowledge
- Quality assurance processes ensuring consistent accuracy
Organizations evaluating whether to maintain in-house coding or partner with service providers should consider the total cost of employment, quality consistency, scalability needs, and access to specialty expertise. Understanding what’s needed to do medical billing and coding successfully helps organizations make informed decisions about resourcing models.
Keeping Current with Regulatory Changes
Medical coding operates in a constantly evolving regulatory environment. Annual ICD-10 updates introduce hundreds of new codes and revise existing ones. CPT code changes reflect new procedures and revised guidelines. Payer policies shift coverage requirements and documentation expectations. Coders must absorb these changes while maintaining productivity and accuracy.
Organizations need structured approaches to manage regulatory changes effectively. Establishing dedicated time for coder education, subscribing to professional coding resources, and implementing systematic review processes help coders stay current. Many practices dedicate the final quarter of each year to preparing for January code updates, reviewing high-volume codes that change, and updating internal coding guidance.
Strategies for managing coding updates:
- Quarterly review sessions covering upcoming regulatory changes
- Subscription to coding newsletters and update services
- Attendance at coding seminars and webinars
- Systematic review of high-volume codes annually
- Documentation of coding policy changes for auditing purposes
Technology platforms can assist with regulatory compliance by automatically updating code databases, implementing new edits, and flagging outdated codes. However, human coders still need education on clinical application of new codes and guidelines to apply changes correctly in practice.
Managing Specialty-Specific Coding Requirements
Different medical specialties present unique coding challenges requiring specialized knowledge. Cardiology coding involves complex bundling rules and extensive modifier usage. Orthopedic coding requires detailed anatomical knowledge and laterality documentation. Behavioral health coding follows different documentation standards and medical necessity criteria. Understanding medical billing for behavioral health illustrates specialty-specific considerations.
Primary care practices handle high volumes with diverse service types, requiring coders who understand evaluation and management guidelines, preventive services, and chronic disease management coding. Surgical specialties demand knowledge of global periods, surgical packages, and modifier 59 usage to avoid inappropriate bundling.
Organizations must decide whether to develop specialty coding expertise internally or access it through partnerships. Small practices may lack sufficient volume in any single specialty to justify dedicated specialty coders, making partnerships more practical. Large multi-specialty groups might maintain specialty-focused coding teams to develop deep expertise.
| Specialty | Primary Coding Challenges | Required Expertise |
|---|---|---|
| Cardiology | Complex bundling edits, extensive modifiers | Cardiovascular anatomy, procedure combinations |
| Orthopedics | Laterality requirements, surgical approaches | Musculoskeletal anatomy, implant coding |
| Radiology | Component billing, professional vs. technical | Imaging modalities, supervision levels |
| Emergency Medicine | Level of service determination, critical care | Time-based coding, bundled services |
Specialty coding expertise directly affects reimbursement levels and compliance risk. Coders who understand specialty-specific nuances capture appropriate revenue while avoiding common errors that trigger denials or audit findings. Organizations should assess their specialty mix and determine the most cost-effective approach to accessing required coding expertise.
Optimizing Coding Performance Through Analytics
Data-driven approaches to coding management enable continuous improvement in accuracy, productivity, and financial outcomes. Organizations that track coding metrics and analyze performance trends identify improvement opportunities and measure the impact of interventions.
Key Performance Indicators for Coding Operations
Effective coding analytics begin with selecting the right metrics to monitor. Organizations should track leading indicators that predict downstream revenue cycle performance and lagging indicators that measure ultimate financial outcomes. The combination provides early warning of problems and validates improvement efforts. Resources on healthcare revenue cycle analytics offer additional insights into performance measurement.
Essential coding KPIs include:
- Coding accuracy rate: Percentage of coded encounters matching audit standards
- Coding productivity: Encounters coded per full-time equivalent per day
- Query rate: Percentage of encounters requiring provider clarification
- Coder-specific error patterns: Individual performance variations
- Denial rates by denial reason: Coding-related versus other denial causes
- Days in coding: Time lag between service delivery and code assignment
Organizations should establish baseline performance levels, set improvement targets, and monitor trends over time. Sudden changes in metrics warrant investigation to identify root causes, whether positive improvements to replicate or negative trends requiring intervention.
Benchmarking against industry standards helps organizations assess relative performance. While absolute benchmarks vary by practice type, specialty mix, and patient complexity, understanding where performance falls relative to peers identifies competitive advantages or improvement needs.
Feedback Loops and Continuous Improvement
Effective coding programs incorporate systematic feedback mechanisms that drive continuous improvement. Regular audits provide objective quality assessments, identifying both strengths to reinforce and weaknesses requiring attention. Sharing audit findings with coders creates learning opportunities and promotes accountability for accuracy.
Productive feedback sessions focus on education rather than punishment. Reviewing challenging cases as a team builds collective expertise and ensures consistent application of coding guidelines. Celebrating high performers and recognizing quality improvements motivates coders and reinforces desired behaviors.
Organizations should implement multiple feedback mechanisms:
- Monthly quality audits sampling coded encounters against standards
- Peer review sessions discussing complex coding scenarios
- Provider education addressing documentation improvement needs
- Denial analysis identifying coding issues requiring remediation
- Performance dashboards tracking individual and team metrics
The most successful coding operations view quality assurance as a learning system rather than a policing function. When coders understand that feedback aims to support their success rather than criticize their work, they engage more productively in improvement efforts. Understanding physician RCM challenges helps coding teams appreciate how their work affects overall practice performance.
Strategic Approaches to RCM Medical Coding
Forward-thinking organizations adopt strategic perspectives on rcm medical coding that extend beyond tactical code assignment. These approaches position coding as a competitive advantage and revenue optimization opportunity rather than merely a compliance requirement.
Proactive Documentation Improvement
Rather than accepting documentation quality as given, leading organizations implement clinical documentation improvement initiatives that engage providers in creating better source material for coding. These programs educate physicians about documentation requirements, provide real-time feedback on common deficiencies, and streamline documentation workflows to reduce provider burden.
CDI specialists review charts concurrent with patient care, identifying documentation gaps that affect code assignment, quality metrics, or risk adjustment. They work directly with providers to obtain additional specificity while patients remain in care, eliminating retrospective queries that delay billing.
Components of successful CDI programs:
- Concurrent chart review during patient episodes of care
- Provider education on documentation requirements and coding impact
- Query templates streamlining communication between CDI and providers
- Metrics tracking documentation improvement and financial impact
- Integration with electronic health record workflows
Organizations investing in CDI typically see improvements in case mix index, quality measure performance, denial rates, and revenue capture. The investment in CDI specialists generates returns through more accurate DRG assignment, better risk adjustment factor scores, and reduced coding queries.
Strategic Partnerships for Coding Excellence
Many healthcare organizations partner with specialized RCM service providers to access coding expertise, scale resources efficiently, and benefit from best practice processes. These partnerships allow organizations to focus internal resources on patient care while leveraging external expertise for revenue cycle operations. Exploring top medical billing companies helps organizations understand partnership options.
Service providers bring economies of scale that individual practices cannot achieve. They invest in technology platforms, maintain certified coding staff, implement quality assurance programs, and stay current with regulatory changes across their client base. This shared infrastructure reduces per-unit costs while maintaining or improving quality compared to in-house operations.
When evaluating potential coding partners, organizations should assess:
| Evaluation Criteria | Why It Matters | Assessment Approach |
|---|---|---|
| Coder Credentials | Ensures baseline competency and compliance | Review certification requirements and ongoing education |
| Quality Assurance | Validates accuracy and identifies improvement needs | Examine audit processes and error remediation approaches |
| Technology Platform | Affects efficiency and integration capabilities | Assess system features and interoperability with practice systems |
| Reporting Capabilities | Enables performance monitoring and improvement | Review sample dashboards and available metrics |
| Industry Experience | Provides relevant expertise for specialty needs | Check references from similar practice types |
Successful partnerships require clear communication, defined performance expectations, and regular performance reviews. Organizations should establish service level agreements specifying accuracy targets, productivity standards, turnaround times, and reporting requirements. Regular meetings reviewing performance against these standards ensure accountability and continuous improvement.
Mastering rcm medical coding fundamentals empowers healthcare organizations to optimize revenue capture, minimize compliance risks, and accelerate cash flow throughout the revenue cycle. The strategic integration of skilled professionals, advanced technology, and data-driven improvement processes creates sustainable competitive advantages in an increasingly complex healthcare environment. Greenhive Billing Solutions provides comprehensive revenue cycle management services that address the full spectrum of coding challenges, from initial documentation review through final payment posting, enabling healthcare providers to focus on patient care while maximizing financial performance through expert billing operations and transparent communication.

