Esophagogastroduodenoscopy with dilation represents a critical therapeutic procedure in gastroenterology, requiring precise coding and documentation to ensure proper reimbursement. Understanding the correct egd with dilation cpt code selection impacts revenue integrity, compliance, and the financial health of gastroenterology practices. Medical billing professionals must navigate specific code definitions, documentation requirements, and payer policies to maximize legitimate reimbursement while maintaining regulatory compliance.
Understanding EGD with Dilation Procedures
Esophagogastroduodenoscopy with dilation involves endoscopic examination of the esophagus, stomach, and duodenum combined with therapeutic expansion of esophageal strictures or narrowing. This procedure addresses conditions such as dysphagia, esophageal strictures, achalasia, and other obstructive pathologies affecting the upper gastrointestinal tract.
The therapeutic component distinguishes these procedures from diagnostic EGD examinations. When physicians perform dilation during an endoscopic procedure, the encounter requires specific procedural codes rather than diagnostic codes alone. This distinction significantly affects reimbursement rates and requires careful attention to documentation specificity.
Clinical Indications for EGD with Dilation
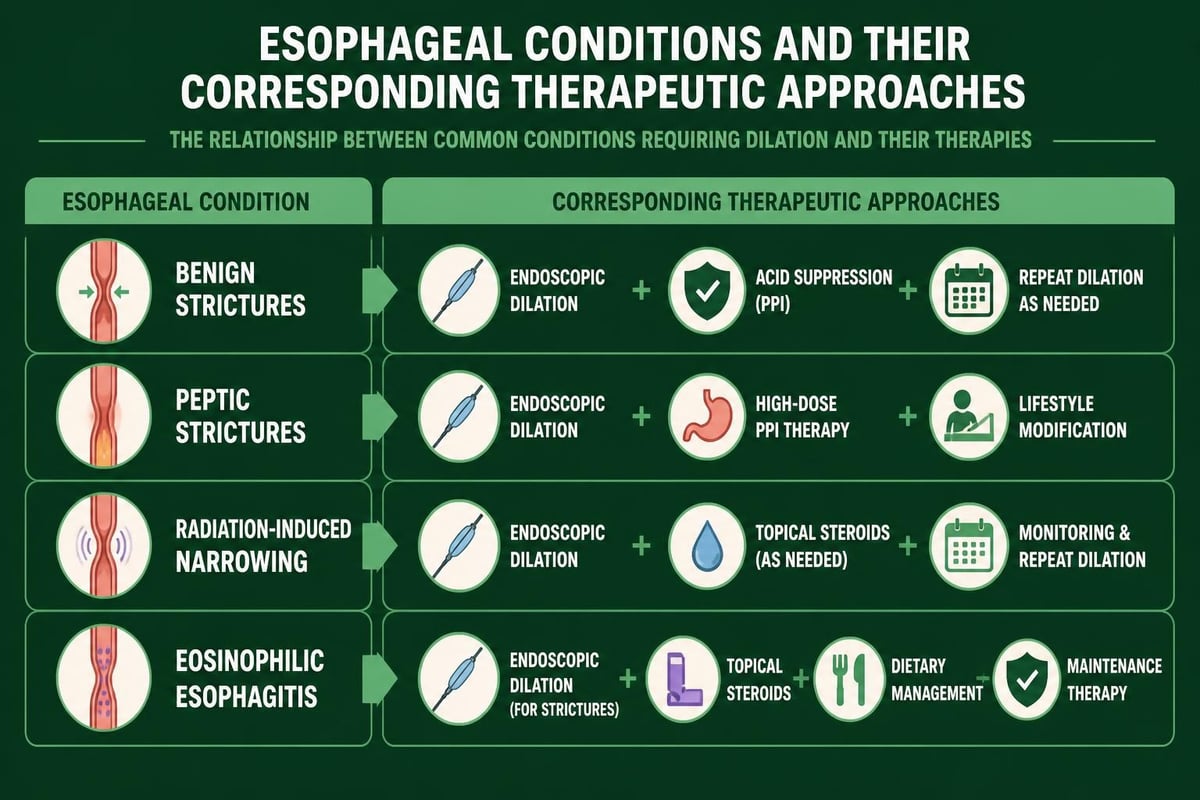
Gastroenterologists perform EGD with dilation for multiple therapeutic purposes:
- Benign esophageal strictures resulting from gastroesophageal reflux disease
- Peptic strictures developing from chronic acid exposure
- Post-surgical strictures following bariatric or esophageal procedures
- Radiation-induced strictures in cancer treatment patients
- Eosinophilic esophagitis causing progressive narrowing
- Schatzki's rings limiting food passage
Proper diagnosis coding supports medical necessity and strengthens claim approval. Each clinical indication requires corresponding ICD-10 codes that justify the therapeutic intervention.
Primary CPT Codes for EGD with Dilation
The egd with dilation cpt code selection depends on specific technical factors, primarily balloon diameter and the use of fluoroscopic guidance. Two primary codes dominate billing for these procedures, each with distinct requirements and reimbursement rates.
CPT Code 43233: Larger Balloon Dilation
The CPT code 43233 applies when physicians perform EGD with dilation of the esophagus using a balloon 30 millimeters or larger in diameter. This code includes fluoroscopic guidance when performed, bundling imaging into the procedural reimbursement.
Key characteristics include:
- Balloon diameter: 30 mm or greater
- Fluoroscopic guidance: Included when performed
- Anatomical target: Esophageal dilation specifically
- Procedure complexity: Higher technical difficulty
This code typically generates higher reimbursement due to the technical complexity and equipment requirements. Providers must document the specific balloon diameter used and any fluoroscopic imaging performed to support code selection.
CPT Code 43249: Smaller Balloon Dilation
The CPT code 43249 describes EGD with transendoscopic balloon dilation of the esophagus using balloons less than 30 millimeters in diameter. This code represents the majority of esophageal dilation procedures performed in gastroenterology practices.
Documentation requirements include:
- Balloon diameter: Less than 30 mm
- Transendoscopic approach: Standard endoscopic technique
- Clinical necessity: Clear indication for therapeutic dilation
- Procedural details: Balloon size, inflation pressure, duration
Understanding the RVU values and Medicare reimbursement rates helps practices forecast revenue and evaluate procedural profitability. These values fluctuate based on geographic location and payer contracts.
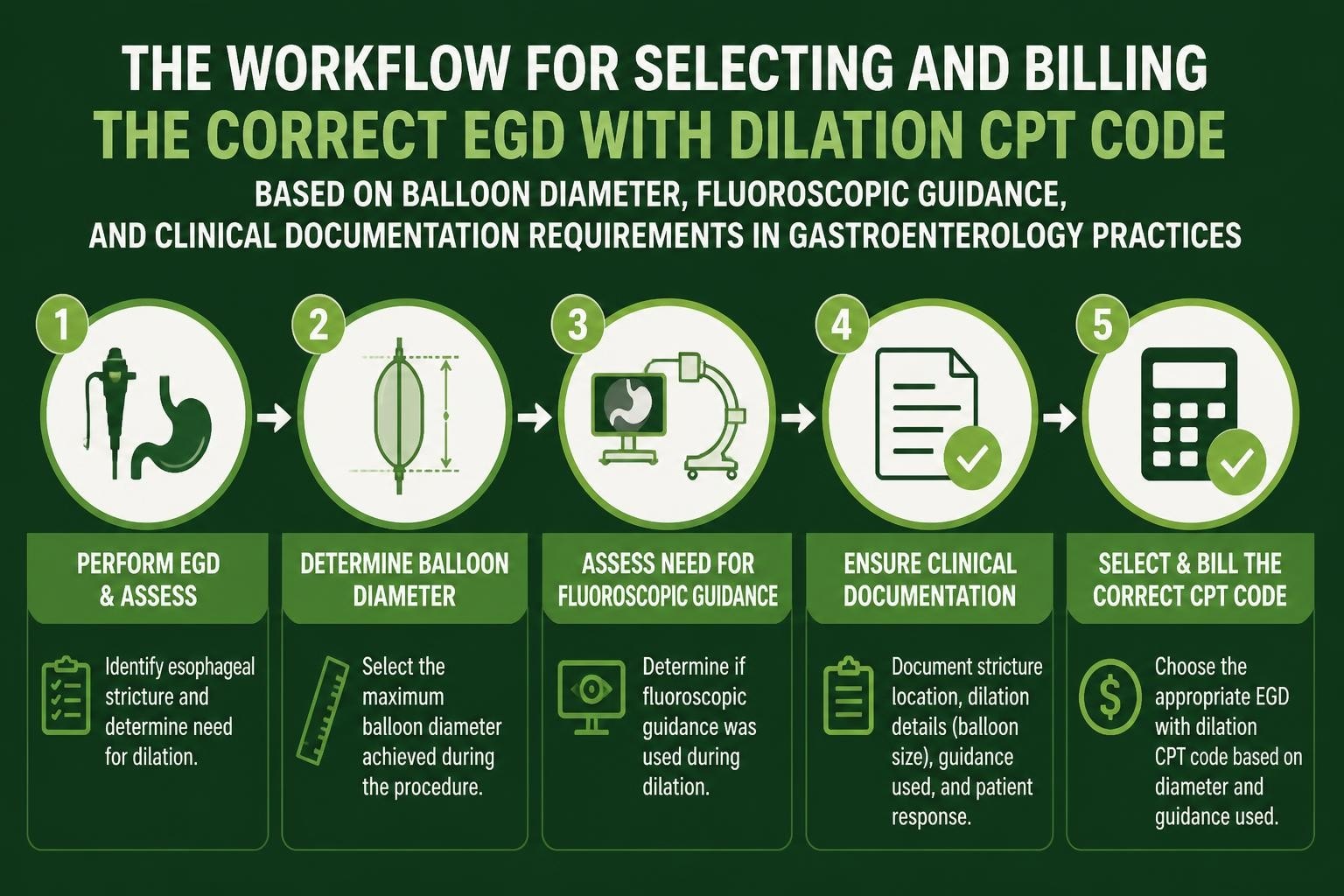
Documentation Requirements for Accurate Coding
Complete procedural documentation forms the foundation of compliant billing for the egd with dilation cpt code. Physicians must provide specific details that support code selection and demonstrate medical necessity.
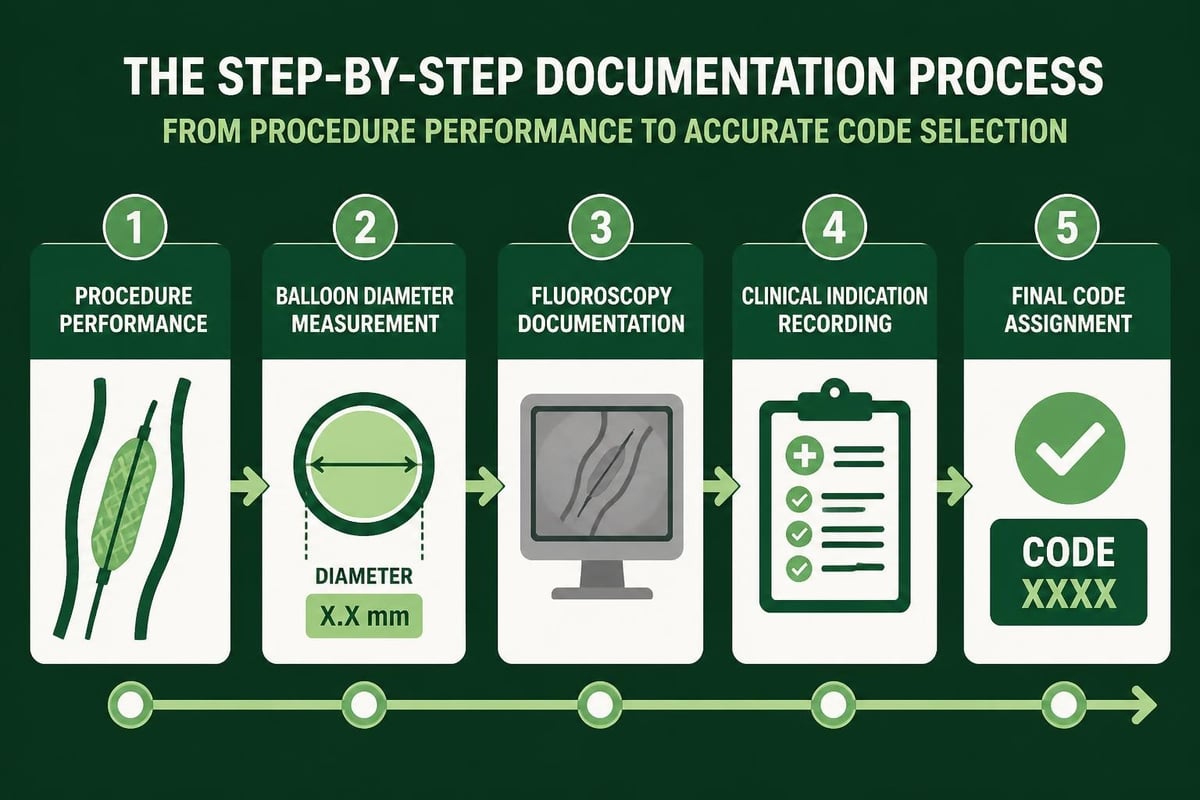
Essential Documentation Elements
Comprehensive operative reports should include these critical components:
| Documentation Element | Required Details | Coding Impact |
|---|---|---|
| Balloon Diameter | Exact measurement in millimeters | Determines code selection |
| Fluoroscopy Use | Whether imaging was performed | Affects CPT 43233 applicability |
| Clinical Indication | Diagnosis requiring dilation | Supports medical necessity |
| Anatomical Location | Specific site of stricture/narrowing | Confirms appropriate code |
| Procedural Outcome | Results of dilation attempt | Validates therapeutic intervention |
The physician's narrative should describe the endoscopic findings, the technical approach to dilation, and any complications or limitations encountered. This detailed documentation protects against audits and supports claim adjudication.
Common Documentation Deficiencies
Billing errors often stem from incomplete or ambiguous documentation. Revenue cycle professionals encounter these frequent deficiencies:
Vague balloon size descriptions: Documentation stating "balloon dilation performed" without specifying diameter prevents accurate code selection. Coders cannot assume balloon size based on clinical context.
Missing fluoroscopy documentation: When physicians use fluoroscopic guidance with larger balloons but fail to document this imaging, practices may lose legitimate reimbursement opportunities.
Incomplete procedural narrative: Generic templates that lack patient-specific details raise red flags during payer review and increase denial risk.
Establishing standardized documentation templates that prompt physicians for required elements improves coding accuracy and reduces claim denials. Many practices integrate structured fields into their electronic health record systems to capture these critical data points.
Navigating Complex Coding Scenarios
Real-world clinical situations frequently present coding challenges that require nuanced understanding of CPT guidelines and payer policies. Expert guidance on EGD dilation coding scenarios helps clarify appropriate code selection.
Multiple Dilation Attempts During Single Encounter
When physicians perform multiple dilation attempts using different balloon sizes during a single procedure, coders must determine whether multiple codes apply or if only the most comprehensive code should be reported.
Step 1: Review the operative report for distinct procedural components and separate anatomical sites.
Step 2: Determine if multiple dilations represent staged approaches to the same stricture or separate therapeutic interventions.
Step 3: Apply appropriate modifiers if billing multiple codes, documenting medical necessity for each component.
Step 4: Verify payer-specific policies regarding multiple procedure reductions and bundling edits.
Generally, when multiple dilations address the same stricture using progressively larger balloons, only the final balloon size determines code selection. However, dilations at separate anatomical locations may support multiple code reporting with appropriate modifiers.
Combining Dilation with Other Endoscopic Procedures
Gastroenterologists frequently perform additional therapeutic interventions during EGD with dilation, such as biopsy, polyp removal, or foreign body extraction. Understanding which procedures bundle and which may be separately reportable affects revenue capture.
The National Correct Coding Initiative establishes bundling relationships between procedural codes. Generally, diagnostic biopsies performed during therapeutic endoscopic procedures are included in the primary procedure code and should not be separately billed.
However, distinct procedural components addressing separate clinical indications may qualify for separate reporting. Practices should consult current coding resources and payer policies to determine appropriate modifier use and code combinations.
Reimbursement Considerations and Revenue Optimization
Understanding reimbursement patterns for the egd with dilation cpt code enables practices to optimize revenue while maintaining compliance. Multiple factors influence payment rates and claim acceptance.
Medicare Payment Methodology
Medicare reimburses EGD with dilation procedures based on the Physician Fee Schedule, which incorporates Relative Value Units (RVUs) adjusted for geographic practice cost differences. The detailed RVU information for CPT 43249 provides insight into payment calculations.
Reimbursement components include:
- Work RVU: Physician time and intensity
- Practice expense RVU: Overhead costs and equipment
- Malpractice RVU: Professional liability insurance
- Geographic adjustment: Location-based cost variations
Private payers typically negotiate contracted rates that may exceed or fall below Medicare rates. Understanding payer-specific fee schedules helps practices forecast revenue and identify profitable procedures.
Denial Prevention Strategies
Proactive denial management protects revenue and reduces administrative burden. Common denial reasons for EGD with dilation claims include:
Medical necessity documentation: Payers may question the appropriateness of dilation without clear documentation of failed conservative management or symptom severity. Comprehensive clinical notes demonstrating prior treatments and objective findings support claim approval.
Incorrect code selection: Balloon diameter discrepancies between documentation and coded procedures trigger audits. Implementing quality reviews before claim submission catches these errors early.
Missing prior authorization: Many payers require advance approval for therapeutic endoscopic procedures. Verifying authorization requirements through eligibility verification services prevents avoidable denials.
Establishing systematic review processes as part of your revenue cycle management process strengthens clean claim rates and accelerates payment cycles.
Modifier Application in EGD with Dilation Billing
Modifiers communicate special circumstances affecting procedure performance or reimbursement. Appropriate modifier use ensures accurate payment while preventing claim rejections.
Common Modifiers for EGD Procedures
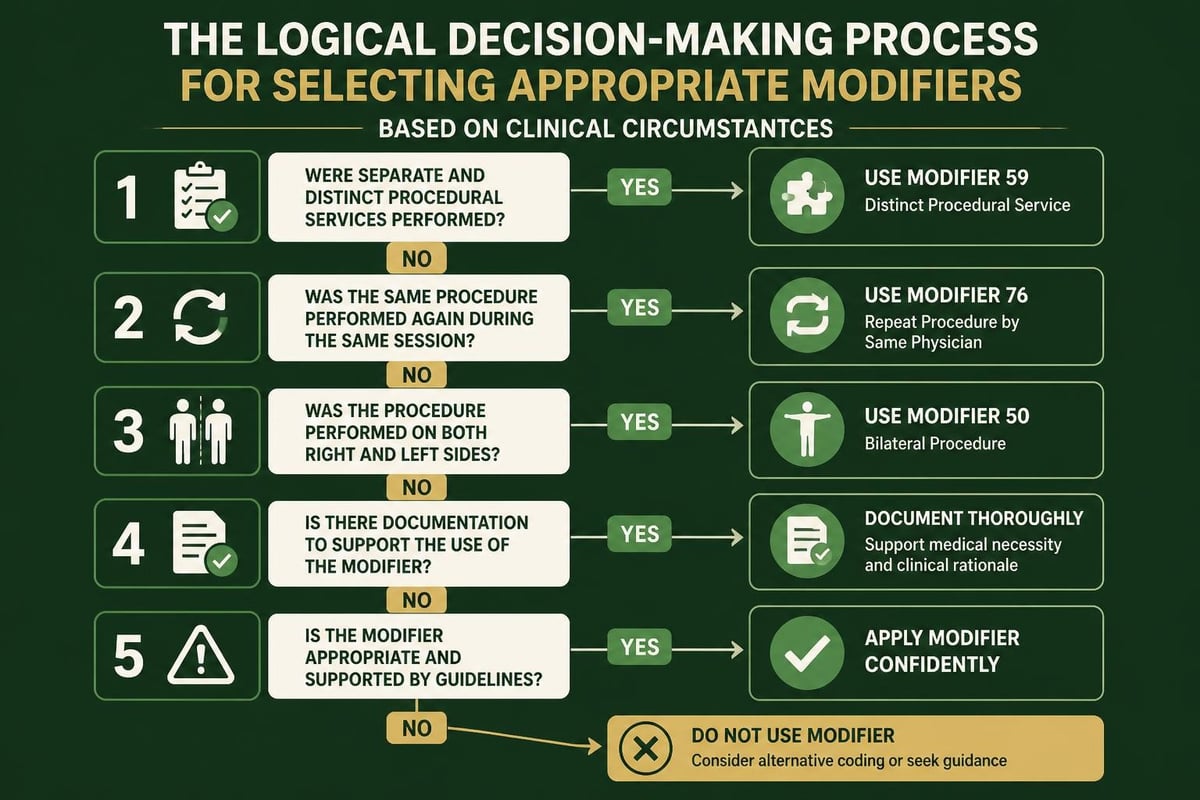
| Modifier | Description | Application Scenario |
|---|---|---|
| 59 | Distinct procedural service | Separate procedure at different site |
| 76 | Repeat procedure by same physician | Subsequent dilation same encounter |
| 77 | Repeat procedure by another physician | Coverage for colleague's patient |
| 78 | Unplanned return to procedure | Complication requiring repeat dilation |
| LT/RT | Left/right side indicators | Bilateral procedures when applicable |
Understanding different types of modifiers in medical billing helps prevent common billing errors and supports claim integrity.
Modifier 59 requires particular caution, as payers scrutinize claims using this modifier for potential unbundling violations. Documentation must clearly demonstrate that procedures represent distinct therapeutic interventions rather than components of a single comprehensive service.
Bilateral Procedure Considerations
While esophageal dilation procedures do not typically involve bilateral anatomical structures, understanding bilateral modifier application remains important for comprehensive endoscopic coding knowledge. Other upper GI procedures may require bilateral modifiers when performed on paired structures.
Compliance and Audit Preparedness
Regulatory scrutiny of endoscopic procedures continues intensifying, making compliance preparedness essential for gastroenterology practices. Understanding audit triggers and maintaining robust documentation protects against financial penalties and reputational damage.
Common Audit Triggers for EGD Procedures
Payers and regulatory agencies target specific patterns that suggest coding irregularities or fraudulent billing:
- Unusually high frequency of therapeutic procedures compared to diagnostic endoscopies
- Consistent use of higher-reimbursing codes without clinical variation
- Lack of medical necessity documentation supporting therapeutic interventions
- Pattern of billing multiple procedures without appropriate modifiers or anatomical distinctions
- Insufficient interval between repeat procedures on the same patient
Practices should conduct internal audits comparing their coding patterns to national benchmarks and identifying statistical outliers requiring review.
Building Audit-Resistant Documentation
Comprehensive documentation strategies create strong defense against audit challenges:
Pre-procedure documentation: Establish medical necessity through symptom documentation, diagnostic test results, and previous treatment failures. This foundation demonstrates that therapeutic intervention represents appropriate clinical management.
Intra-procedure documentation: Detailed operative reports describing specific technical approaches, equipment used, and procedural findings provide objective evidence supporting code selection.
Post-procedure documentation: Follow-up notes demonstrating symptomatic improvement or continued clinical need for additional interventions complete the clinical narrative.
Implementing physician education programs ensures clinical staff understand documentation requirements and the connection between complete notes and appropriate reimbursement. Many practices find that investing in documentation improvement yields significant revenue enhancement without increasing procedural volume.
ICD-10 Coding for Medical Necessity Support
Proper diagnosis coding establishes medical necessity and justifies the egd with dilation cpt code. Linking appropriate ICD-10 codes to procedural codes strengthens claims and reduces denial risk.
Primary Diagnosis Codes for Esophageal Dilation
Common diagnosis codes supporting EGD with dilation include:
- K22.2: Esophageal obstruction
- K22.3: Perforation of esophagus
- K22.4: Dyskinesia of esophagus
- K22.70: Barrett's esophagus without dysplasia
- K22.81: Esophageal polyp
- K21.0: Gastroesophageal reflux disease with esophagitis
The specific diagnosis code selected should reflect the documented clinical condition requiring therapeutic intervention. Generic or symptom-based codes may not adequately support medical necessity for therapeutic procedures.
Linking Diagnoses to Procedures
Establishing clear relationships between diagnoses and procedures strengthens claim validity. The operative report should explicitly reference the clinical condition being addressed through the therapeutic intervention.
For example, when performing dilation for a peptic stricture, the documentation should describe the stricture location, degree of narrowing, and how this anatomical finding relates to the patient's presenting symptoms. This narrative creates logical progression from diagnosis through treatment selection to procedural performance.
Understanding what is a CPT code for insurance in healthcare claims provides broader context for how procedural and diagnosis coding interact within the claims process.
Payer-Specific Policies and Coverage Criteria
Individual payers establish unique policies governing coverage for EGD with dilation procedures. Familiarity with these variations prevents claim denials and supports efficient revenue cycle operations.
Medicare Local Coverage Determinations
Medicare Administrative Contractors publish Local Coverage Determinations that outline covered indications, frequency limitations, and documentation requirements for endoscopic procedures in their jurisdictions. These policies vary by geographic region, requiring practices to understand their specific MAC's requirements.
Common Medicare coverage criteria include:
Documented dysphagia: Patients must demonstrate swallowing difficulty through clinical evaluation or diagnostic testing before therapeutic dilation receives coverage approval.
Failed conservative management: Many LCDs require evidence of attempted medical management before approving therapeutic interventions. Documentation should reflect dietary modifications, medication trials, or other conservative approaches.
Appropriate interval between procedures: Repeat dilations within short timeframes may trigger medical review. Practices should document continued clinical need and rationale for repeat interventions.
Commercial Payer Requirements
Private insurance companies often establish more restrictive policies than Medicare, including:
- Prior authorization mandates requiring approval before procedure scheduling
- Specific provider credentialing limiting which physicians may perform procedures
- Facility requirements designating approved procedure locations
- Documentation submission demanding operative reports before payment
Effective denial management in medical billing requires understanding these payer-specific variations and implementing processes to address requirements proactively.
Technology Integration for Coding Accuracy
Modern practice management systems and electronic health records offer tools that enhance coding accuracy and streamline documentation workflows. Leveraging these technologies improves efficiency while reducing error rates.
Clinical Decision Support Systems
Advanced EHR platforms incorporate clinical decision support that prompts physicians for required documentation elements during procedure notes. These systems can:
- Alert providers when balloon diameter documentation is missing
- Suggest appropriate ICD-10 codes based on documented clinical findings
- Flag potential coding errors before claim submission
- Integrate coding guidelines directly into documentation workflows
This real-time guidance prevents common documentation deficiencies that lead to coding errors and claim denials.
Computer-Assisted Coding Tools
Some practices implement computer-assisted coding software that analyzes operative reports and suggests appropriate CPT codes based on documented procedures. While human oversight remains essential, these tools provide valuable coding support and quality assurance.
The AHA Coding Clinic guidance on EGD balloon dilation represents authoritative coding direction that many CAC systems incorporate into their logic.
Staff Training and Education Strategies
Maintaining coding accuracy requires ongoing education for clinical and billing staff. Gastroenterology practices should implement structured training programs addressing procedural coding, documentation requirements, and regulatory updates.
Physician Documentation Training
Clinical providers need education on how their documentation directly impacts coding accuracy and reimbursement. Effective training programs should:
Use real examples: Present actual operative reports from the practice, highlighting both strong documentation and areas for improvement. This concrete approach makes abstract coding concepts tangible for physicians.
Quantify revenue impact: Demonstrate how documentation improvements translate to appropriate reimbursement increases. Physicians respond to data showing financial benefits of complete documentation.
Simplify requirements: Create reference tools that physicians can quickly consult during documentation, such as laminated cards listing required elements for common procedures.
Provide feedback loops: Share coding outcomes with physicians, explaining when documentation prevented accurate coding or led to denials.
Billing Staff Competency Development
Coding professionals require regular updates on egd with dilation cpt code guidelines, payer policy changes, and emerging compliance issues. Professional development strategies include:
- Industry certification maintenance through continuing education credits
- Regular coding audits with feedback and corrective action plans
- Payer policy reviews summarizing coverage changes
- Case study discussions exploring complex coding scenarios
Investing in staff development reduces coding errors, improves first-pass claim acceptance rates, and strengthens revenue cycle performance. Understanding comprehensive billing code information supports ongoing learning.
Quality Metrics and Performance Monitoring
Establishing key performance indicators for EGD with dilation coding enables practices to track accuracy, identify improvement opportunities, and benchmark against industry standards.
Critical Coding Metrics
| Metric | Target Range | Significance |
|---|---|---|
| Clean claim rate | >95% | First-pass acceptance without edits |
| Coding accuracy rate | >98% | Correct code selection validated by audit |
| Average reimbursement per procedure | Payer-specific | Revenue optimization indicator |
| Denial rate for EGD procedures | <5% | Effectiveness of documentation and coding |
| Days in accounts receivable | <30 days | Revenue cycle efficiency |
Regular monitoring of these metrics identifies trends requiring intervention and validates improvement initiatives.
Benchmark Comparison Analysis
Comparing practice performance to national and regional benchmarks provides context for evaluating coding effectiveness. Significant deviations from expected patterns warrant investigation to determine whether documentation, coding, or clinical practice variations explain differences.
Practices performing substantially higher percentages of therapeutic procedures compared to diagnostic endoscopies should ensure documentation clearly establishes medical necessity for this case mix. Conversely, unusually low therapeutic procedure rates might indicate missed revenue opportunities through under-coding.
Managing Evolving Coding Guidelines
CPT codes, coding guidelines, and payer policies continuously evolve, requiring practices to maintain current knowledge and adapt workflows accordingly. Systematic approaches to guideline monitoring prevent costly errors resulting from outdated practices.
Annual CPT Updates
The American Medical Association publishes annual CPT code updates that may affect endoscopic procedure coding. Changes include:
- New codes introduced for emerging procedures
- Revised code descriptors clarifying appropriate use
- Deleted codes requiring transition to alternative codes
- Modified guidelines affecting code selection logic
Practices should review annual updates before implementation, assessing how changes affect their specific procedure mix and revenue projections.
Regulatory and Compliance Updates
Beyond coding changes, practices must monitor regulatory developments affecting EGD procedures, including HIPAA privacy requirements, fraud and abuse enforcement priorities, and quality reporting mandates.
Establishing responsibility for regulatory monitoring ensures no critical updates fall through administrative cracks. Many practices designate a compliance officer or engage external consultants to track and communicate relevant changes.
Accurate selection and billing of the egd with dilation cpt code requires comprehensive understanding of procedural variations, documentation requirements, and payer policies. Implementing systematic approaches to coding accuracy, staff training, and compliance monitoring protects revenue while ensuring regulatory adherence. Greenhive Billing Solutions provides expert revenue cycle management services that help gastroenterology practices optimize coding accuracy, reduce denials, and maximize legitimate reimbursement for complex procedures. Our experienced team stays current with evolving coding guidelines and payer requirements, allowing physicians to focus on patient care while we handle the complexities of revenue cycle management.

