Understanding modifier 25 in medical billing is essential for healthcare providers who want to maximize legitimate reimbursements while maintaining compliance. This critical billing modifier allows providers to report a significant, separately identifiable evaluation and management (E/M) service on the same day as a procedure or other service. Despite its straightforward definition, modifier 25 remains one of the most frequently audited and misunderstood modifiers in medical billing. Healthcare practices that master its proper application can improve revenue capture, reduce claim denials, and minimize audit risks.
What Modifier 25 Represents in Medical Billing
Modifier 25 in medical billing serves a specific purpose: it indicates that an E/M service performed on the same day as a procedure was significant and separately identifiable from the procedural component. According to guidance from the American Medical Association, this modifier should only be applied when the E/M service goes beyond the typical pre-procedural and post-procedural work associated with the primary service.
The Centers for Medicare & Medicaid Services (CMS) established modifier 25 to recognize that patients sometimes require additional evaluation beyond what is normally included in a procedure's global package. This creates a billing scenario where both services deserve separate reimbursement.
Key Characteristics That Define Proper Usage
When examining modifier 25 in medical billing scenarios, several characteristics must be present for appropriate application:
- The E/M service must be significant in nature, addressing a condition or concern beyond the procedure itself
- Documentation must clearly demonstrate the separately identifiable nature of the E/M encounter
- The E/M service may be prompted by the same diagnosis or a different condition
- The modifier attaches to the E/M code, not the procedure code
- Both services must occur on the same calendar day
Documentation Requirements for Modifier 25 Compliance
Proper documentation forms the foundation of defensible modifier 25 claims. The American Academy of Family Physicians emphasizes that documentation must clearly show why the E/M service was necessary beyond the routine care associated with the procedure.
Healthcare providers should ensure their clinical notes include these critical elements:
Chief Complaint and History
Every modifier 25 claim should document a distinct reason for the patient encounter. The chief complaint should reflect the additional concern that prompted the E/M service. If the patient presents for both a routine procedure and an unrelated acute issue, the documentation must clearly delineate between these two purposes.
Examination Findings
The physical examination should extend beyond what is minimally necessary to perform the planned procedure. Document specific findings related to the additional clinical concern. Simply repeating the same examination elements required for the procedure does not support modifier 25 usage.
Medical Decision-Making
Perhaps most importantly, documentation must demonstrate the complexity of medical decision-making involved in the E/M service. This includes differential diagnoses, treatment options considered, medication adjustments, and clinical reasoning that goes beyond procedural planning.
| Documentation Component | Insufficient for Modifier 25 | Sufficient for Modifier 25 |
|---|---|---|
| Chief Complaint | "Patient here for injection" | "Patient here for scheduled injection; also reports new onset chest pain for 3 days" |
| Examination | "Knee examined, effusion noted" | "Knee examined for injection; cardiovascular exam performed due to chest pain concerns, revealing irregular rhythm" |
| Decision-Making | "Proceed with injection" | "Injection performed for arthritis; separately evaluated chest pain, ordered EKG, adjusted cardiac medications, scheduled follow-up" |
Common Scenarios Appropriate for Modifier 25
Understanding when modifier 25 in medical billing applies helps providers recognize legitimate opportunities for proper billing. The American College of Cardiology provides specific guidance on appropriate modifier 25 scenarios within cardiology practices, principles that extend across specialties.
Scenario 1: Scheduled Procedure with Unrelated Acute Issue
A patient arrives for a scheduled lesion removal on their arm but also reports severe headaches that started two days ago. The provider performs a comprehensive evaluation of the headache including neurological examination, reviews medication history, and develops a treatment plan. The lesion removal proceeds as scheduled. This scenario justifies modifier 25 because the headache evaluation represents significant, separately identifiable work.
Scenario 2: Procedure Decision Made During E/M Service
A patient presents with abdominal pain. During the E/M service, the provider performs a detailed history and physical examination, reviews prior records, and determines that joint aspiration is medically necessary based on findings. The provider performs the aspiration during the same visit. This represents appropriate modifier 25 usage because the E/M service was significant and led to the decision to perform the procedure.
Scenario 3: Chronic Condition Management Plus Procedure
A diabetic patient comes for their scheduled diabetic foot care procedure. During the same visit, the provider also evaluates recent blood glucose readings, adjusts insulin dosages, addresses new diabetic neuropathy symptoms, and counsels the patient on dietary modifications. The separately identifiable diabetic management constitutes an E/M service distinct from the foot procedure.
Important Note: Same-diagnosis scenarios require extra scrutiny. The E/M service must still be significant and separately identifiable, even when addressing the same condition that prompted the procedure.
Five Critical Mistakes to Avoid with Modifier 25
Healthcare providers commonly make specific errors when applying modifier 25 in medical billing. Recognizing these mistakes helps practices implement stronger compliance measures through effective denial management strategies.
Mistake 1: Applying Modifier 25 to Minor Pre-Procedural Work
The most frequent error involves adding modifier 25 to every E/M service performed on the same day as a procedure, regardless of whether the E/M was truly significant. Pre-procedural assessment, patient positioning, consent discussions, and routine post-procedural checks are bundled into the procedure code and do not warrant separate E/M billing.
Mistake 2: Inadequate Documentation
Claims may be denied even when modifier 25 is clinically appropriate if documentation fails to support the billing. Generic templates that do not clearly distinguish the E/M service from procedural work create audit vulnerabilities. Many providers struggle with medical coding services that accurately reflect the clinical scenario.
Mistake 3: Confusion with Other Modifiers
Modifier 25 specifically applies to E/M services performed with procedures. Other modifiers serve different purposes:
- Modifier 24: E/M service during a post-operative period unrelated to the original procedure
- Modifier 57: E/M service that resulted in the decision for surgery (for major procedures)
- Modifier 59: Distinct procedural service (does not apply to E/M codes)
Understanding different types of modifiers in medical billing prevents inappropriate substitutions.
Mistake 4: Routine Follow-Up Billed as Separate E/M
When a patient returns for a scheduled procedure related to a previous visit's diagnosis, providers sometimes bill both the procedure and an E/M with modifier 25 without documenting new findings or additional complexity. Unless new symptoms, complications, or unrelated conditions arise, routine follow-through on a previously established treatment plan does not support modifier 25.
Mistake 5: Ignoring Payer-Specific Policies
Different insurance carriers maintain varying policies regarding modifier 25 acceptance. Some payers scrutinize certain code combinations more closely or have specific documentation requirements. The Journal of Urgent Care Medicine highlights how payer policies impact modifier 25 claims, particularly in urgent care settings.
Step-by-Step Guide for Correct Modifier 25 Application
Healthcare practices benefit from standardized processes that ensure consistent, compliant modifier 25 usage. Follow this systematic approach:
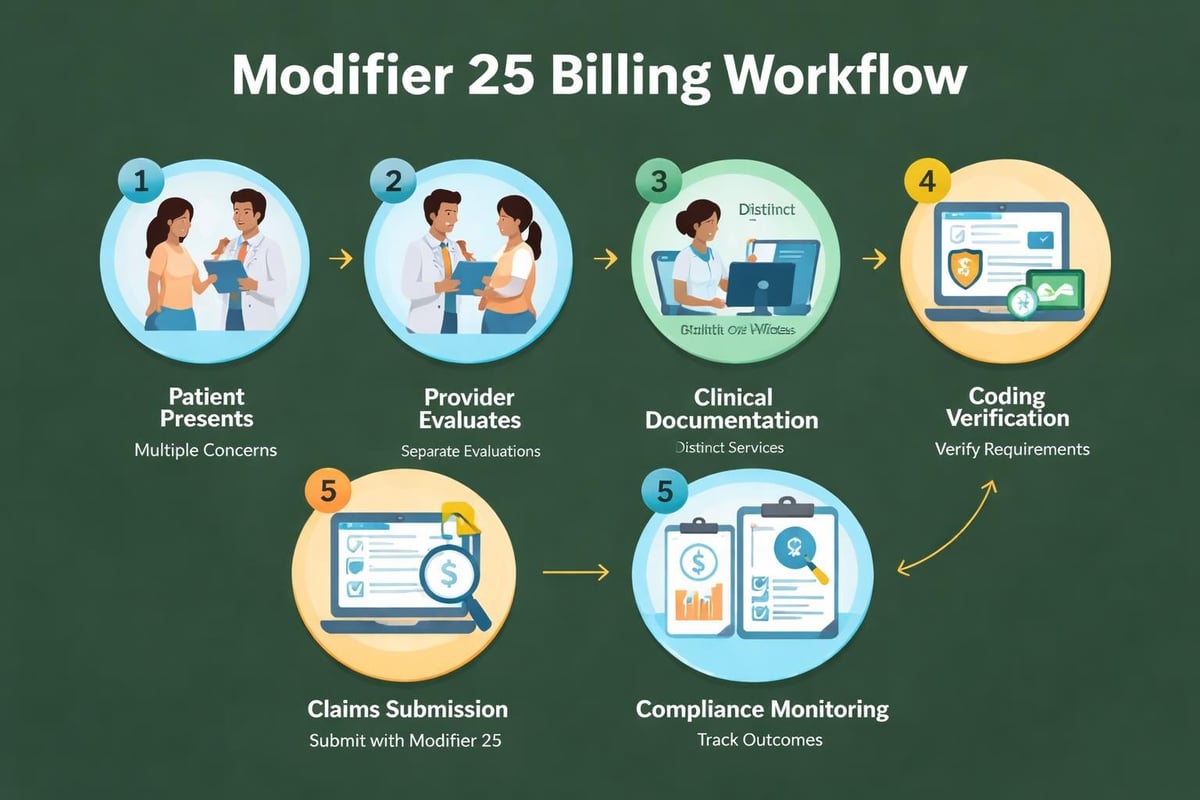
Step 1: Verify Service Timing
Confirm that both the E/M service and the procedure occurred on the same calendar day. Modifier 25 does not apply to services performed on different dates, even within a global period.
Step 2: Assess E/M Significance
Evaluate whether the E/M service involved substantial work beyond the procedure's typical components. Ask: "Would this E/M service have been performed if the patient had not undergone the procedure?" If yes, modifier 25 may be appropriate.
Step 3: Confirm Separate Identifiability
Ensure the E/M service addressed different aspects of patient care than the procedure itself. The clinical documentation should clearly delineate between the two services without overlap or redundancy.
Step 4: Review Documentation Completeness
Before claim submission, verify that documentation includes all required E/M components (history, examination, medical decision-making) and clearly demonstrates the service's separate nature. Many practices implementing healthcare revenue cycle analytics track modifier 25 denial patterns to identify documentation weaknesses.
Step 5: Apply Modifier Correctly
Append modifier 25 to the E/M code only, not to the procedure code. Enter the E/M code with modifier 25 on one claim line and the procedure code without modifier 25 on a separate line.
Step 6: Monitor Claim Outcomes
Track modifier 25 claim acceptance rates, denial reasons, and audit requests. This ongoing monitoring through medical claim submission services helps identify patterns requiring process adjustments.
Payer Audits and Modifier 25 Defense Strategies
Insurance carriers frequently audit modifier 25 claims due to historical overuse across the healthcare industry. Understanding audit triggers and defense strategies protects practice revenue.
Common Audit Triggers
Payers may flag claims for review based on these patterns:
- High frequency of modifier 25 usage compared to specialty benchmarks
- Specific code combinations with historically high abuse rates
- Same-diagnosis E/M and procedure pairings
- Providers who consistently bill modifier 25 with particular procedure codes
- Random selection for general compliance review
Building a Defensible Position
When facing a modifier 25 audit, practices should compile comprehensive documentation packages that include:
- Complete medical records showing the full clinical encounter
- Clear highlighting of E/M elements separate from procedural notes
- Explanation letters describing the clinical rationale for both services
- References to payer policies and CMS guidelines supporting proper usage
- Evidence of provider training on modifier 25 compliance
Net Health’s analysis demonstrates that practices with robust documentation protocols experience significantly higher success rates in audit defense.
Training Staff for Modifier 25 Compliance
Successful modifier 25 implementation requires coordinated efforts between clinical and administrative staff. Revenue cycle management excellence depends on everyone understanding their role.
Provider Education
Physicians, nurse practitioners, and physician assistants must understand documentation standards that support modifier 25 claims. Regular training should cover:
- Clinical scenarios that warrant modifier 25 usage
- Documentation templates that clearly separate E/M from procedural work
- Common denial reasons and how to avoid them
- Payer-specific requirements that affect billing decisions
Coding Staff Competency
Medical coders serve as the final checkpoint before claim submission. Their responsibilities include:
| Coder Responsibility | Implementation Strategy |
|---|---|
| Documentation Review | Verify that clinical notes support modifier 25 before adding it to claims |
| Provider Queries | Return incomplete documentation with specific questions about E/M significance |
| Compliance Monitoring | Track modifier 25 usage patterns and alert management to potential issues |
| Education Feedback | Communicate common documentation deficiencies to providers for improvement |
Working with experienced medical billing services ensures that coding staff have the expertise needed for complex modifier decisions.
Front Office Awareness
Reception and scheduling staff should understand basic modifier 25 concepts to improve visit documentation from the start. When scheduling appointments where both an E/M service and procedure may occur, staff should note both purposes clearly in the appointment details.
Industry Resources and Continued Learning
Staying current with modifier 25 policies requires ongoing education as regulations and payer requirements evolve. Healthcare practices should leverage multiple resources:
Professional organizations like Reenix Excellence provide detailed E/M coding guidance with practical examples applicable to daily practice situations. These resources complement internal training programs and help standardize approaches across the organization.
Many practices also benefit from subscribing to coding newsletters, attending webinars focused on E/M services, and participating in peer discussion forums where billing professionals share experiences and solutions. Understanding CPT codes for insurance provides essential context for modifier application.
Additionally, comprehensive accounting resources offer financial perspectives on modifier 25 that help practice managers understand the revenue impact of proper usage.
Technology and Modifier 25 Optimization
Modern revenue cycle management increasingly relies on technology solutions that flag potential modifier 25 opportunities and compliance risks. While individual practices may not develop proprietary software, partnering with experienced billing service providers who utilize advanced tools offers significant advantages.
Electronic health record (EHR) systems can be configured with templates that prompt providers to document E/M elements when procedures are scheduled. Smart alerts can notify coders when documentation may support modifier 25 or when additional clarification is needed.
Analytics platforms track modifier 25 acceptance rates by payer, procedure type, and provider, identifying patterns that inform training priorities and process improvements. These capabilities, when managed by skilled medical coding audit services professionals, transform raw data into actionable compliance strategies.
Financial Impact of Proper Modifier 25 Usage
The revenue implications of modifier 25 in medical billing extend beyond individual claim values. Practices that consistently apply this modifier appropriately experience multiple financial benefits:
Increased Legitimate Revenue Capture
Many providers unknowingly leave money on the table by failing to recognize valid modifier 25 scenarios. When documentation supports separate E/M billing and providers perform significant work, modifier 25 ensures appropriate compensation for services rendered.
Reduced Denial and Rework Costs
Improper modifier 25 usage creates costly denial cycles requiring appeals, resubmissions, and administrative time. Clean claims submitted correctly the first time improve cash flow and reduce overhead expenses associated with claim management.
Decreased Audit Liability
Practices with compliant modifier 25 processes face lower risks of payer audits and the potential takebacks that accompany audit failures. This financial predictability supports better practice management and planning.
Enhanced Payer Relationships
Consistent compliance demonstrates billing integrity to insurance carriers, potentially reducing overall scrutiny and improving contract negotiations. Payers view practices with low error rates more favorably during credentialing and contract renewals.
Modifier 25 Across Different Specialties
While modifier 25 principles remain consistent across medicine, different specialties encounter unique scenarios that require specialized knowledge.
Primary Care Applications
Family medicine and internal medicine practices frequently use modifier 25 when addressing multiple chronic conditions during a visit that also includes a procedure like joint injection, lesion removal, or minor surgery. The comprehensive nature of primary care often creates legitimate modifier 25 opportunities.
Surgical Specialty Considerations
Surgical specialists must carefully distinguish between pre-operative evaluations that justify modifier 25 versus those requiring modifier 57 for major surgeries. Minor procedures more commonly pair with modifier 25 when additional unrelated conditions are addressed.
Dermatology and Dermatologic Surgery
Dermatology practices performing numerous lesion removals must ensure that modifier 25 claims reflect truly significant E/M work, such as full-body skin cancer screenings or management of systemic skin conditions, rather than simple lesion identification.
Cardiology and Specialized Medicine
Cardiologists and other specialists performing diagnostic and therapeutic procedures must document the medical complexity that warrants separate E/M billing. Managing multiple cardiac conditions while performing echocardiograms or stress tests can support modifier 25 when properly documented.
Understanding these specialty-specific nuances becomes particularly important for practices utilizing medical billing services for small practices that may lack internal specialty expertise.
Medicare, Medicaid, and Commercial Payer Variations
Modifier 25 policies vary across payer types, requiring practices to maintain current knowledge of multiple requirements.
Medicare Guidelines
Medicare's modifier 25 policy generally follows CMS documentation guidelines, accepting the modifier when E/M services are significant and separately identifiable. Medicare Administrative Contractors (MACs) may issue local coverage determinations that affect specific procedure and E/M code combinations.
Medicaid Programs
State Medicaid programs maintain individual policies regarding modifier 25 acceptance. Some states impose more restrictive requirements or limit modifier 25 usage with certain procedure codes. Practices serving Medicaid populations must understand state-specific rules.
Commercial Insurance Carriers
Private payers implement varying modifier 25 policies, from liberal acceptance matching Medicare standards to restrictive approaches requiring pre-authorization or additional documentation. Some carriers maintain edit systems that automatically deny specific code combinations regardless of documentation quality.
Maintaining awareness of these payer differences represents a significant challenge that many practices address through partnerships with specialized billing providers offering comprehensive eligibility verification services and payer-specific expertise.
Mastering modifier 25 in medical billing requires comprehensive understanding of clinical documentation requirements, compliance standards, and payer-specific policies. Healthcare practices that implement systematic processes for modifier 25 application, maintain thorough documentation, and provide ongoing staff education position themselves for optimal revenue capture while minimizing audit risks. Greenhive Billing Solutions helps healthcare providers navigate these complexities through expert revenue cycle management services that ensure compliant, accurate modifier 25 usage tailored to each practice's specialty and payer mix, maximizing legitimate reimbursements while protecting against compliance risks.

