Medical billing modifiers serve as critical communication tools between healthcare providers and insurance payers, providing essential context about the services rendered. These two-character codes, when appended to CPT or HCPCS codes, clarify specific circumstances surrounding a procedure, identify variations in service delivery, and prevent claim denials. Understanding and correctly applying modifiers represents a fundamental skill for revenue cycle management professionals, directly impacting reimbursement rates and cash flow stability. Having access to a comprehensive list of modifiers in medical billing reference materials helps billing teams maintain accuracy and compliance while reducing errors that lead to rejected claims.
Understanding the Role of Modifiers in Revenue Cycle Management
Modifiers play an indispensable role in the healthcare billing ecosystem. They communicate critical information that CPT codes alone cannot convey, such as whether a procedure was bilateral, performed by multiple surgeons, or conducted in an unusual location.
Without proper modifier usage, claims often face automatic denials or downcoding, both of which negatively impact practice revenue. A complete guide to medical billing modifiers demonstrates how these codes prevent misinterpretation and ensure payers understand the exact nature of services provided.
The financial implications extend beyond individual claims. Systematic modifier errors create patterns that trigger audits, delay payments, and erode payer relationships. Healthcare providers who invest in proper training and maintain updated reference materials see measurably better claim acceptance rates.
Why Healthcare Providers Need Reliable Modifier References
Medical billing teams face constant pressure to maintain accuracy while processing high claim volumes. The complexity increases as coding guidelines evolve annually, with modifiers being added, retired, or redefined based on regulatory changes.
Maintaining current knowledge requires dedication and resources. Many practices struggle with staff turnover, making consistent training challenging. This reality makes having a dependable list of modifiers in medical billing documentation essential for operational continuity.
Key benefits of maintaining comprehensive modifier references include:
- Reduced claim denial rates due to coding errors
- Faster reimbursement cycles through first-pass claim acceptance
- Improved compliance with payer-specific requirements
- Enhanced audit defense with proper documentation
- Streamlined training for new billing staff members
Understanding denial management in medical billing helps organizations recognize how modifier errors contribute to revenue leakage and develop preventive strategies.
Comprehensive Table of Essential Medical Billing Modifiers
The following table represents the most frequently used modifiers across multiple specialties, providing billing professionals with quick reference information for daily operations.
| Modifier | Description | Primary Use Case |
|---|---|---|
| 22 | Increased Procedural Services | When procedure requires significantly greater work than typically required |
| 24 | Unrelated Evaluation and Management Service | E/M service during postoperative period for different diagnosis |
| 25 | Significant, Separately Identifiable E/M Service | Same-day E/M service and procedure by same physician |
| 26 | Professional Component | Professional portion only of service with technical component |
| 50 | Bilateral Procedure | Procedure performed on both sides during same session |
| 51 | Multiple Procedures | Multiple procedures performed during same session |
| 52 | Reduced Services | Service/procedure partially reduced or eliminated at physician discretion |
| 53 | Discontinued Procedure | Procedure terminated due to extenuating circumstances |
| 54 | Surgical Care Only | Surgeon performs operative procedure only |
| 55 | Postoperative Management Only | Provider performs postoperative care only |
| 56 | Preoperative Management Only | Provider performs preoperative care only |
| 57 | Decision for Surgery | E/M service resulted in decision for surgery |
| 58 | Staged or Related Procedure | Procedure during postoperative period was planned/related |
| 59 | Distinct Procedural Service | Identifies procedures that are not normally reported together |
| 62 | Two Surgeons | Two surgeons performing different parts of single procedure |
| 76 | Repeat Procedure by Same Physician | Same physician repeats procedure on same day |
| 77 | Repeat Procedure by Another Physician | Different physician repeats procedure on same day |
| 78 | Unplanned Return to Operating Room | Related procedure during postoperative period |
| 79 | Unrelated Procedure During Postoperative Period | Procedure performed during postoperative period of another procedure |
| 80 | Assistant Surgeon | Assistant surgeon services |
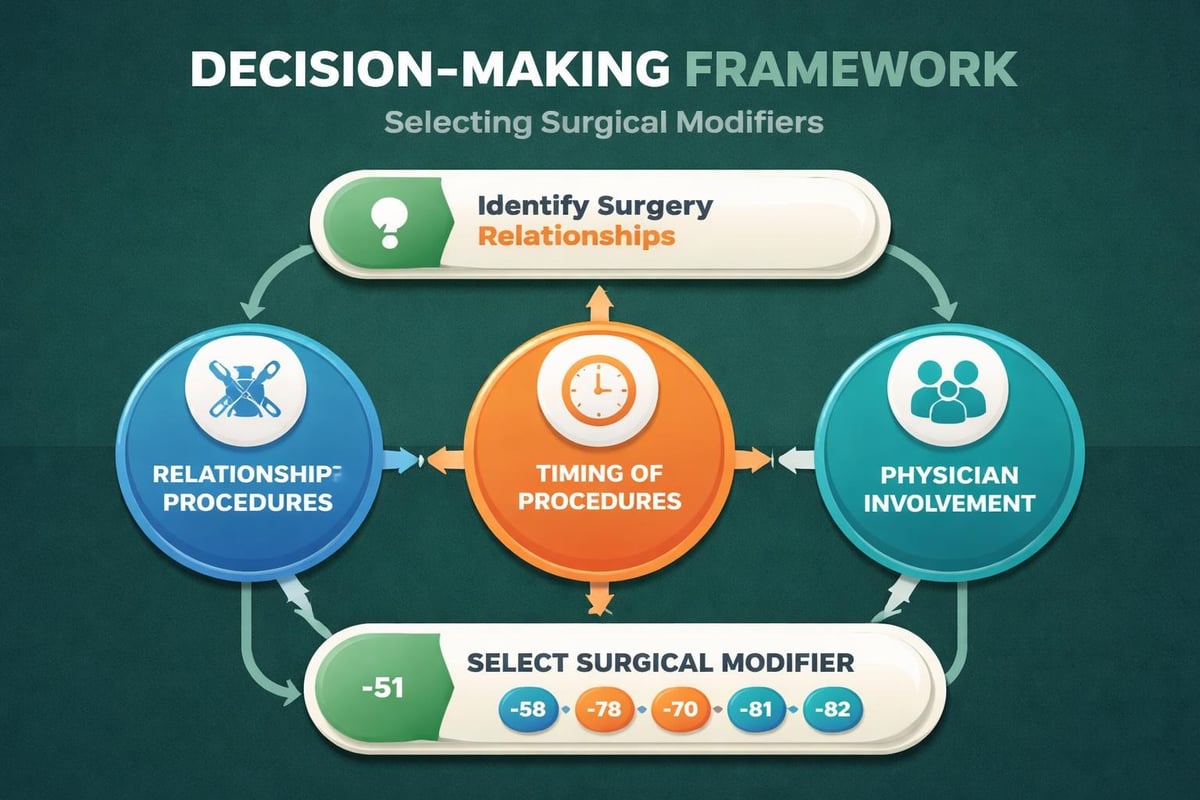
Critical Modifiers for Surgical and Procedural Billing
Surgical billing presents unique challenges requiring precise modifier application. The distinction between planned and unplanned procedures, multiple surgeon scenarios, and staged operations demands careful attention to documentation and coding practices.
Understanding HCPCS modifiers expands knowledge beyond CPT modifiers, particularly for durable medical equipment, ambulance services, and specific payer requirements.
Multiple Procedure Modifiers: 51 vs 59
Modifier 51 indicates multiple procedures performed during the same session, typically resulting in payment reduction for additional procedures. Insurance companies apply this modifier to recognize efficiency gains when procedures share operative time and resources.
Conversely, modifier 59 errors represent one of the most audited areas in medical billing. This modifier signals distinct procedural services that are not typically reported together but are appropriate under specific circumstances.
Appropriate uses for modifier 59 include:
- Different anatomical sites or organ systems
- Different patient encounters on the same date
- Separate incisions or excisions
- Separate lesions or injuries
- Procedures not ordinarily performed together
The Centers for Medicare & Medicaid Services introduced X{EPSU} modifiers to provide more specificity than modifier 59, though many commercial payers still primarily recognize the original code.
Evaluation and Management Modifiers That Impact Reimbursement
Evaluation and Management services constitute significant revenue for most practices, making proper modifier application crucial for appropriate payment. The interplay between E/M services and procedures on the same date creates frequent coding challenges.
Modifier 25 allows separate payment for significant, separately identifiable E/M services provided on the same day as a procedure or other service. Documentation must clearly demonstrate the E/M service exceeded the usual pre- and post-service work associated with the procedure.
Documentation Requirements for Modifier 25
Payers scrutinize modifier 25 claims intensively due to historical overuse. Successful claims require documentation that establishes the E/M service as distinct from the procedural service.
The medical record should demonstrate a separate patient complaint or condition necessitating evaluation beyond the procedure's inherent requirements. Simply performing a cursory examination before a planned procedure does not justify modifier 25.
| Modifier | When to Apply | Documentation Must Show |
|---|---|---|
| 24 | E/M during global period | Unrelated to original procedure; different diagnosis |
| 25 | E/M same day as procedure | Significant, separately identifiable service |
| 27 | Multiple outpatient E/M encounters | Separate encounter on same date |
| 57 | Decision for major surgery | E/M resulted in surgery decision within 24 hours |
Understanding what is a CPT code for insurance provides foundational knowledge for applying modifiers correctly, as modifiers modify the base CPT code's meaning.
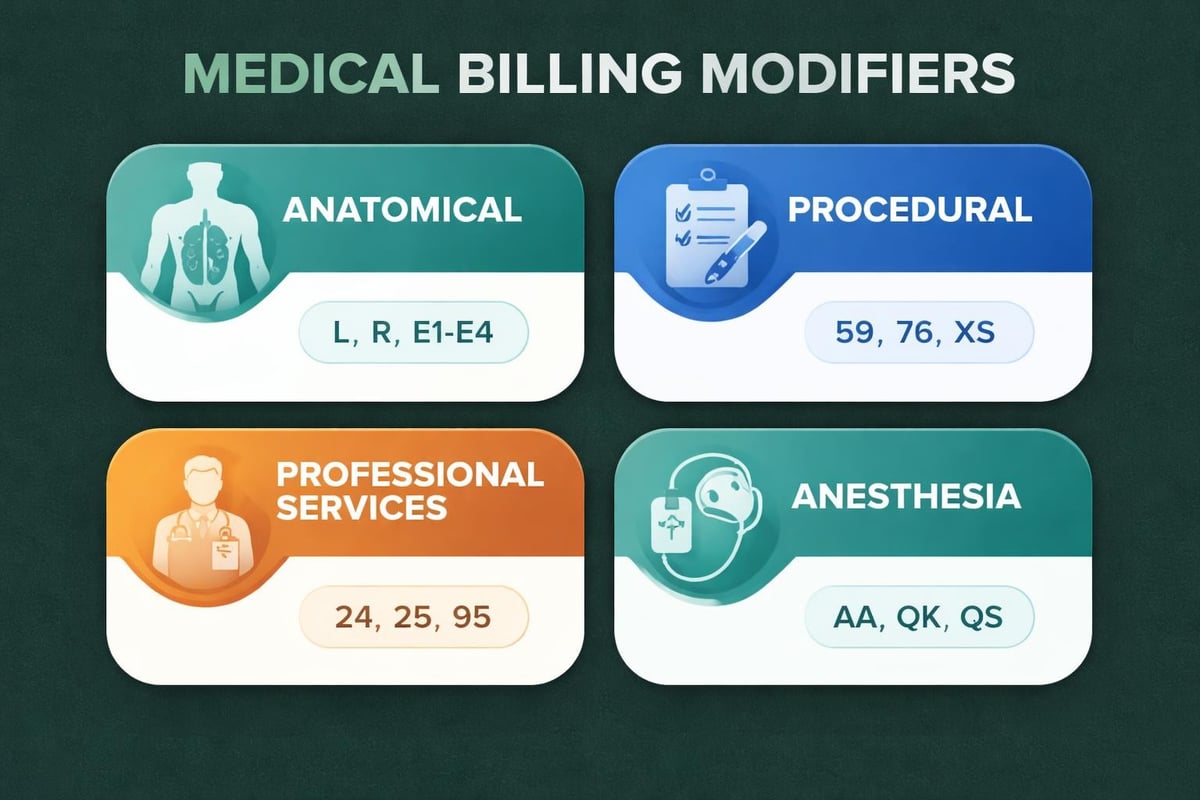
Anatomical and Laterality Modifiers for Precise Billing
Anatomical modifiers specify the exact location of services, preventing ambiguity in claim processing. These modifiers become particularly important when providers perform services on paired organs or extremities.
Modifier 50 indicates bilateral procedures performed during the same operative session. However, payer policies vary significantly regarding bilateral modifier usage and reimbursement methodologies.
Common anatomical modifiers include:
- LT (Left side): Procedure performed on left side of body
- RT (Right side): Procedure performed on right side of body
- 50 (Bilateral): Identical procedure performed on both sides
- E1-E4: Upper eyelid modifiers (right/left, upper/lower)
- F1-F9, FA: Finger modifiers identifying specific digits
- T1-T9, TA: Toe modifiers identifying specific digits
The complexity increases when coding for ophthalmology, podiatry, and orthopedic procedures where precise anatomical identification affects reimbursement. Many payers require separate line items for bilateral procedures rather than accepting modifier 50.
Professional vs Technical Component Modifiers
Many diagnostic and imaging services contain both professional and technical components, each with distinct billing requirements. The professional component represents the physician's interpretation and reporting, while the technical component covers equipment, supplies, and technician services.
Modifier 26 indicates only the professional component is being billed, appropriate when the provider interprets studies performed at separate facilities. Conversely, modifier TC (technical component) identifies equipment and technician services without professional interpretation.
Common Scenarios for Component Modifiers
Hospital-based radiologists frequently use modifier 26 when interpreting studies for hospital outpatients, as the hospital bills the technical component separately. This split billing ensures appropriate payment distribution between facility and professional services.
Independent diagnostic testing facilities must understand these distinctions to avoid duplicate billing or revenue leakage. The absence of appropriate modifiers often results in incorrect payments requiring refunds or appeals.
Working with revenue cycle management services helps practices navigate these complexities and ensure accurate component billing across all service lines.
Anesthesia and Assistant Surgeon Modifiers
Anesthesia services utilize specific modifiers indicating provider type and unusual circumstances. These modifiers affect both reimbursement amounts and medical necessity determinations.
| Modifier | Anesthesia Application | Reimbursement Impact |
|---|---|---|
| 23 | Unusual Anesthesia | Services typically not requiring anesthesia |
| 47 | Anesthesia by Surgeon | Surgeon provides regional/general anesthesia |
| AA | Anesthesiologist | Anesthesiologist personally performs service |
| QK | Medical Direction (2-4 concurrent) | Anesthesiologist directing CRNA services |
| QX | CRNA with Medical Direction | CRNA under anesthesiologist supervision |
| QZ | CRNA without Medical Direction | CRNA working independently |
Assistant surgeon modifiers (80, 81, 82, AS) indicate varying levels of surgical assistance, each with different reimbursement percentages. Modifier 80 represents standard assistant surgeon services, typically reimbursed at 16% of the surgeon's fee.
Modifier 82 applies when an assistant surgeon is medically necessary but a qualified surgeon is unavailable, often in rural or underserved areas. Documentation must justify the medical necessity and unavailability of regular assistant surgeons.
Maintaining Accuracy With Updated Modifier References
The healthcare billing landscape evolves continuously, with annual CPT code updates, payer policy changes, and regulatory modifications affecting modifier usage. Maintaining current references ensures compliance and optimal reimbursement.
A comprehensive list of modifiers in medical billing reference materials should include not only the modifier codes and descriptions but also payer-specific guidelines and documentation requirements. Consulting resources like commonly used modifiers helps teams stay current with industry standards.
Creating Internal Reference Materials
Beyond accessing external resources, successful billing departments develop internal guidelines tailored to their specialty mix and payer contracts. These customized references incorporate specialty-specific modifier applications and document historical denial patterns.
Internal reference materials should include real-world examples from the practice, making training more relevant and immediately applicable. Regular staff meetings reviewing challenging claims reinforces proper modifier selection and improves overall coding accuracy.
Elements of effective internal modifier references:
- Specialty-specific modifier applications with examples
- Payer-specific requirements and preferences
- Documentation templates supporting modifier usage
- Denial analysis highlighting common modifier errors
- Regular update schedules aligned with coding changes
Understanding types of modifiers in medical billing provides framework for organizing internal resources by functional category rather than simple alphabetical listing.
Payer-Specific Modifier Requirements and Variations
While standard modifier definitions remain consistent, payer policies regarding modifier acceptance and reimbursement vary significantly. Medicare maintains the most standardized approach, but commercial payers often implement unique requirements.
Some payers reject modifier 50 entirely, requiring providers to bill bilateral procedures on separate lines with RT and LT modifiers. Others accept modifier 50 but apply different reimbursement methodologies, paying 100% for one side and 50% for the second, or applying different percentage calculations.
Medicare vs Commercial Payer Differences
Medicare's policies regarding modifiers serve as industry standards, but commercial payers frequently deviate based on contract negotiations and internal policies. The National Correct Coding Initiative (NCCI) edits guide Medicare modifier usage, particularly for modifier 59 and its X{EPSU} variants.
Commercial payers may not recognize X{EPSU} modifiers, requiring continued use of modifier 59 despite Medicare's preference for more specific codes. This variation necessitates payer-specific training and reference materials.
Accessing HCPCS and CPT modifier lists provides foundational understanding of standard modifier definitions and HIPAA compliance guidelines applicable across payers.
Training Staff on Proper Modifier Application
Effective modifier usage requires comprehensive training programs addressing both technical knowledge and practical application. New billing staff need structured onboarding covering fundamental modifier concepts, while experienced staff benefit from ongoing education on updates and complex scenarios.
Coding certifications provide valuable foundations, but specialty-specific training addresses unique modifier applications in particular practice settings. Orthopedic practices face different modifier challenges than primary care offices, requiring tailored educational approaches.
Developing Competency Through Case Studies
Real-world case studies transform abstract modifier rules into practical applications. Reviewing actual claims, both successful and denied, helps staff understand the consequences of modifier decisions and develop critical thinking skills.
Regular coding audits identify patterns of errors and knowledge gaps, informing targeted training initiatives. This data-driven approach ensures training addresses actual deficiencies rather than covering generic content.
Organizations exploring what billing and coding specialists do recognize how specialized knowledge directly impacts financial performance and why investing in ongoing education yields measurable returns.
Common Modifier Errors and Prevention Strategies
Despite comprehensive training and reference materials, certain modifier errors occur with concerning frequency across healthcare organizations. Recognizing these common pitfalls enables implementation of targeted prevention strategies.
Frequent modifier errors include:
- Using modifier 25 for minor E/M services that don't meet "significant, separately identifiable" threshold
- Applying modifier 59 when more specific X{EPSU} modifiers are appropriate
- Billing modifier 50 to payers requiring separate line items with RT/LT modifiers
- Omitting required modifiers for bilateral procedures or assistant surgeons
- Appending modifiers in incorrect sequence when multiple modifiers apply
Prevention strategies combine technology solutions with human oversight. Claims scrubbing software can identify missing or inappropriate modifiers based on coded procedures, but experienced coders must evaluate clinical documentation to confirm proper application.
Understanding healthcare revenue cycle analytics enables practices to track modifier-related denial patterns and measure improvement following intervention strategies.
Technology Solutions Supporting Modifier Management
Modern practice management and billing systems incorporate modifier logic, alerting users to missing or potentially inappropriate modifier applications. These automated checks serve as valuable safety nets, though they cannot replace human judgment based on clinical documentation review.
Advanced systems integrate payer-specific edits, automatically applying correct modifier sequencing and flagging combinations that trigger automatic denials. This intelligence reduces manual research time and improves first-pass acceptance rates.
| Technology Solution | Modifier Support Features | Implementation Consideration |
|---|---|---|
| Practice Management Systems | Built-in modifier prompts, payer-specific rules | Requires configuration for specialty and payer mix |
| Claims Scrubbing Software | Pre-submission validation, NCCI edit checking | Must update regularly for coding changes |
| Encoder Software | Modifier suggestions based on documentation | Effectiveness depends on documentation quality |
| Revenue Cycle Analytics | Denial tracking by modifier, trend identification | Requires dedicated analysis resources |
Integration between electronic health records and billing systems enables automatic modifier suggestions based on clinical documentation, though verification remains essential. The most sophisticated systems learn from historical patterns, improving recommendations over time.
Audit Preparation and Modifier Compliance
Auditors scrutinize modifier usage intensively, as inappropriate modifiers represent potential improper payments. Preparing for audits requires demonstrating systematic processes for modifier selection and comprehensive documentation supporting each application.
Internal compliance programs should include regular modifier-focused audits, particularly for high-risk codes like modifiers 22, 25, and 59. These proactive reviews identify issues before external auditors discover them, allowing corrective action and staff retraining.
Documentation Standards Supporting Modifier Defense
Successful audit defense begins with documentation created at the point of service. Physicians and advanced practice providers must understand how their documentation supports or contradicts modifier usage, making them partners in compliance efforts.
Templates and prompts within EHR systems can guide providers toward documentation that satisfies modifier requirements. For modifier 25, templates should prompt providers to clearly document the separate nature of E/M services performed alongside procedures.
Reviewing common CPT code modifiers helps auditors and billing teams maintain consistent understanding of proper applications across various clinical scenarios.
Modifier Resources for Ongoing Reference and Learning
Beyond maintaining internal reference materials, billing professionals benefit from accessing authoritative external resources for complex modifier questions and updates. Multiple organizations provide comprehensive modifier guidance, though quality and currency vary.
Professional associations like AAPC and AHIMA offer continuing education focused on modifier applications, often including specialty-specific sessions addressing unique challenges. These educational opportunities provide networking with peers facing similar coding dilemmas.
Online resources range from free government publications to subscription-based commercial services. Medicare's online resources, including the Medicare Learning Network, provide authoritative guidance on modifier policies affecting all government payers.
Building a personal library of trusted resources, both print and digital, enables quick reference during daily coding activities. Bookmarking reliable websites and maintaining organized files of payer policies creates efficiency and reduces research time.
Having a well-organized list of modifiers in medical billing materials accessible to all team members ensures consistency across the department and reduces individual staff members' stress when encountering unfamiliar scenarios.
Specialty-Specific Modifier Considerations
Different medical specialties encounter unique modifier challenges based on their typical procedure mix and payer relationships. Orthopedic practices routinely use anatomical modifiers and modifier 50 for bilateral procedures, while radiology practices focus heavily on professional and technical component modifiers.
Specialty-specific modifier priorities:
- Orthopedics: Anatomical modifiers (RT, LT, FA, T1-T9), modifier 50, modifier 59 for multiple procedures
- Radiology: Modifiers 26 and TC, modifier 59 for multiple imaging studies
- Surgery: Modifiers 22, 50, 51, 62, 80 for complex and team-based procedures
- Primary Care: Modifiers 24, 25, 57 for evaluation and management services
- Pathology: Modifiers 26 and TC, modifier 91 for repeat laboratory tests
Tailoring training and reference materials to specialty-specific applications improves relevance and retention. Generic modifier education often fails to address the specific scenarios staff encounter daily, reducing practical value.
Understanding different types of medical coding within specialty contexts helps billing professionals appreciate how modifiers integrate with broader coding frameworks.
Mastering modifier usage requires commitment to ongoing education, access to current reference materials, and systematic quality assurance processes. Healthcare organizations that prioritize modifier accuracy see measurable improvements in claim acceptance rates, reduced denials, and faster reimbursement cycles. Greenhive Billing Solutions brings specialized expertise in revenue cycle management, helping healthcare providers navigate complex modifier requirements while maintaining compliance and maximizing reimbursements. Our comprehensive services include expert coding review, denial management, and staff training designed to optimize your practice's financial performance.

