The healthcare financial landscape continues to evolve at a rapid pace, creating both challenges and opportunities for medical practices nationwide. Understanding the dynamics of the revenue cycle management industry has become essential for healthcare providers seeking to maintain financial stability while delivering quality patient care. This comprehensive examination explores market trends, technological advancements, outsourcing patterns, and strategic considerations that shape how healthcare organizations optimize their revenue operations.
Understanding the Revenue Cycle Management Industry Landscape
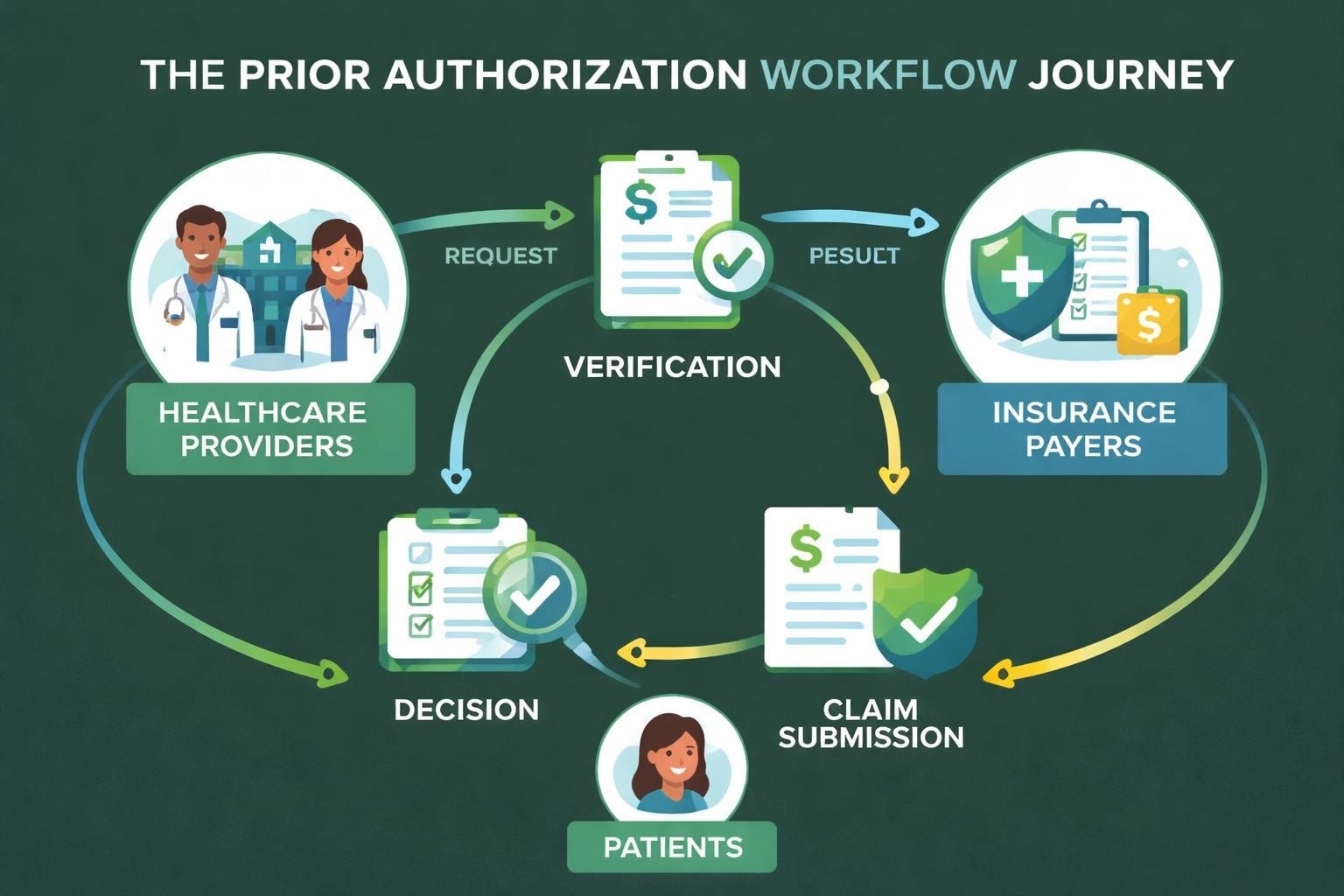
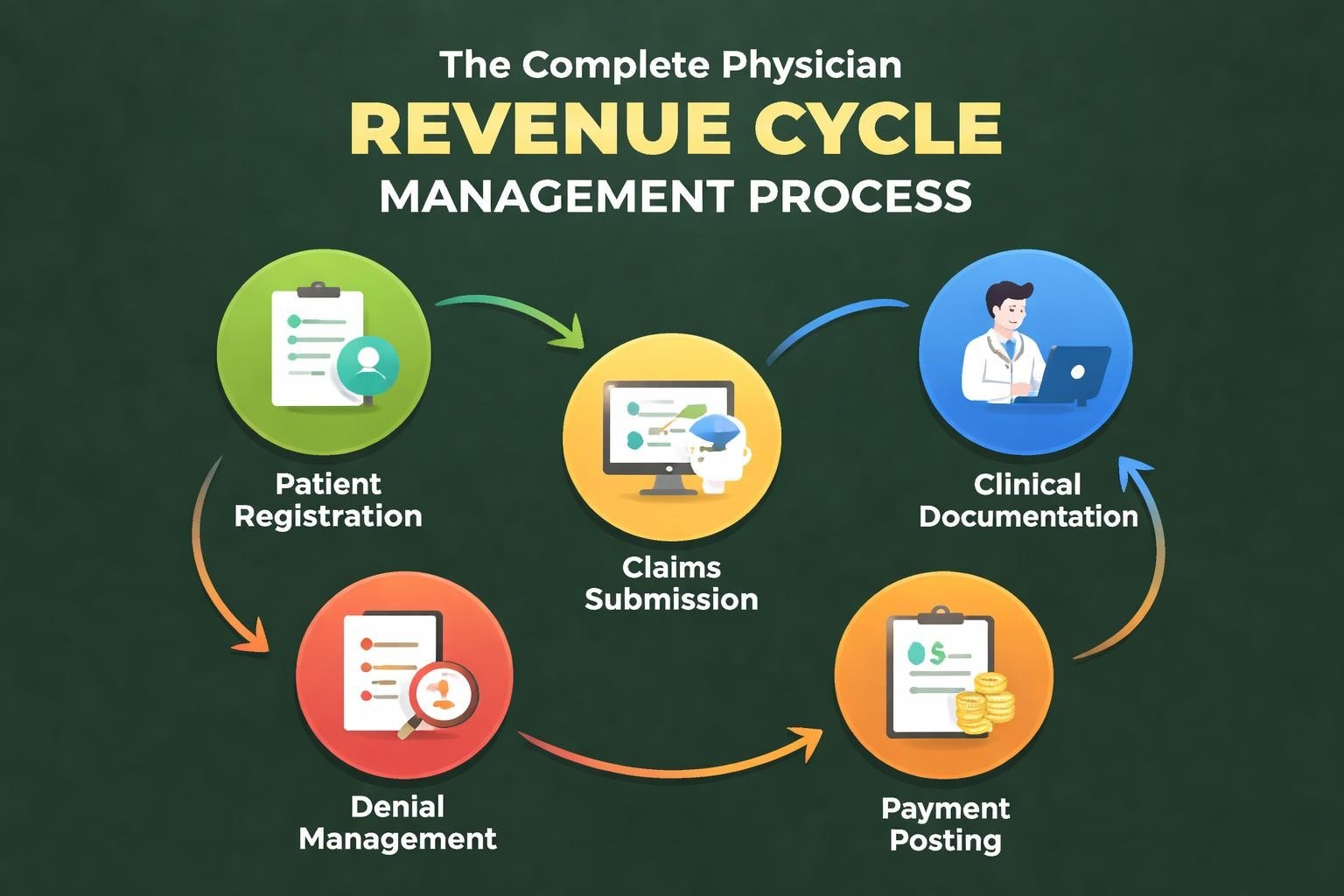
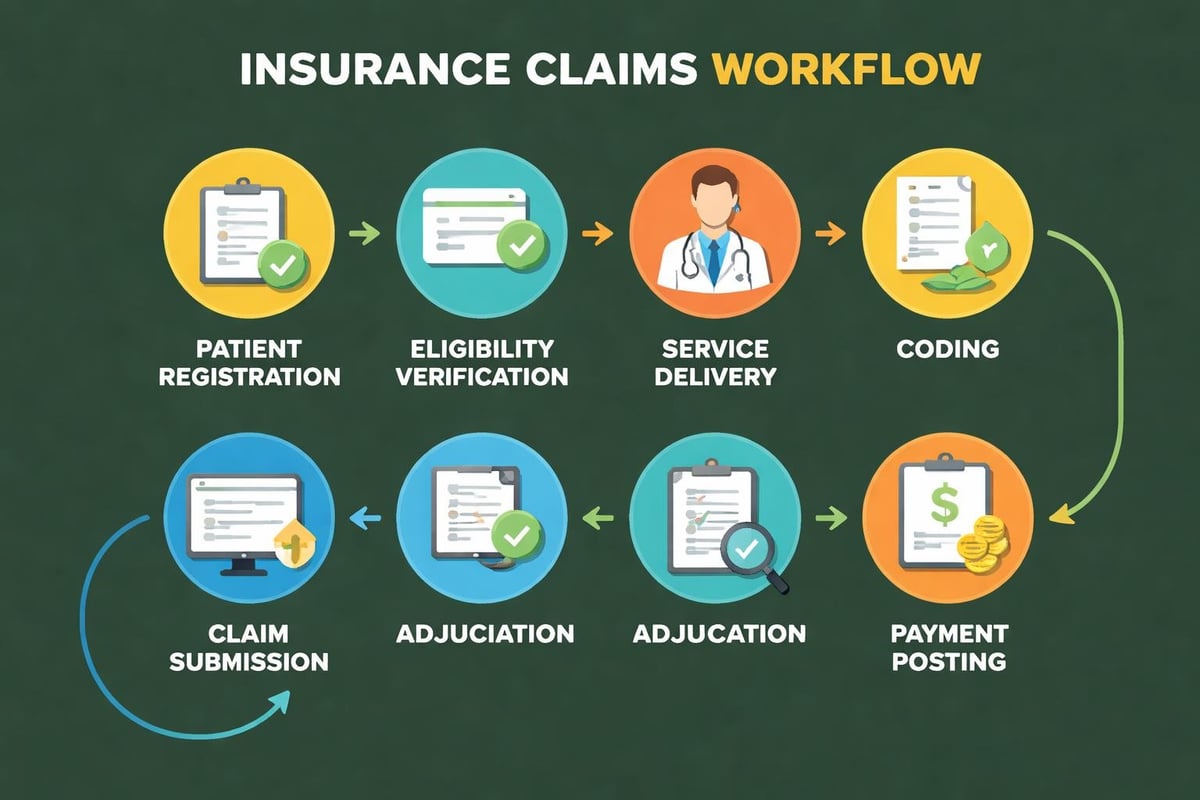
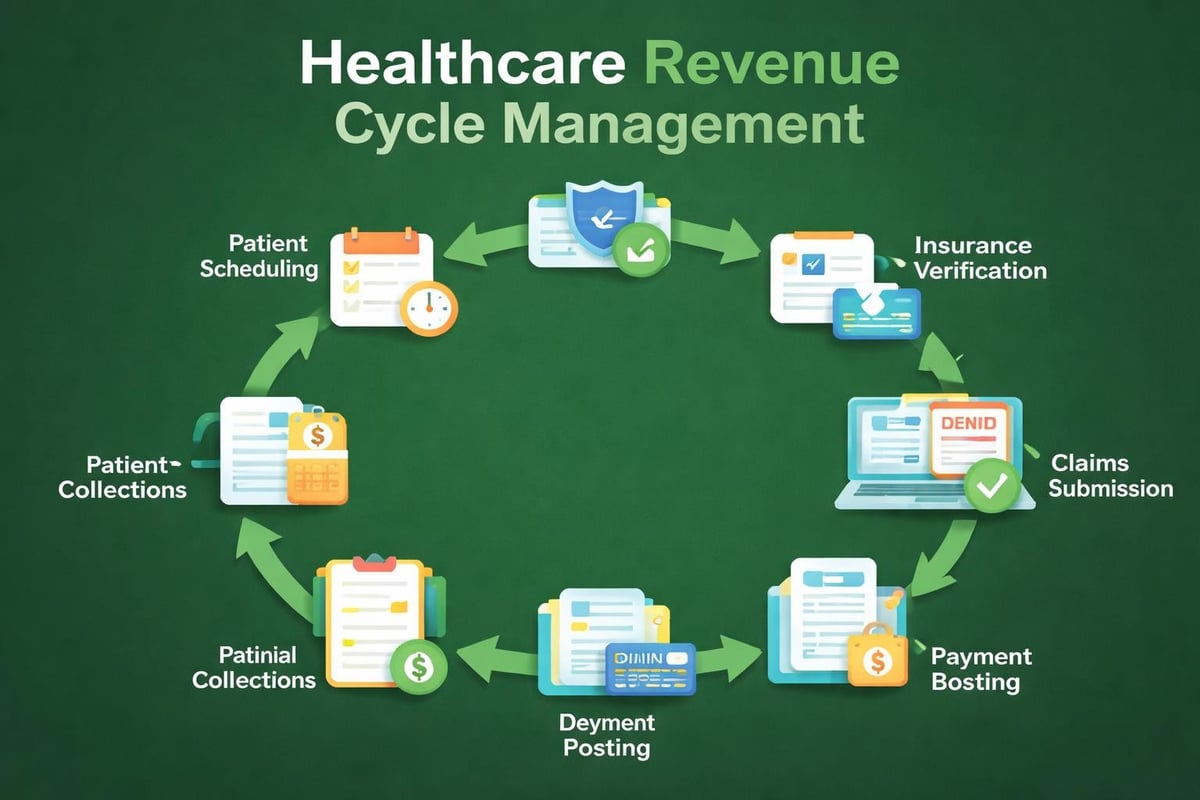
The revenue cycle management industry represents a critical segment of healthcare operations, encompassing all administrative and clinical functions that contribute to capturing, managing, and collecting patient service revenue. This sector has experienced significant transformation over the past decade, driven by regulatory changes, technological innovation, and shifting reimbursement models.
Market analysts project substantial growth for the revenue cycle management industry through the end of the decade. According to industry research, the global market continues expanding as healthcare organizations recognize the value of specialized expertise in managing complex billing processes. This growth reflects increasing demand for services that reduce administrative burden while improving collection rates.
Healthcare providers face mounting pressure to optimize every aspect of their financial operations. The complexity of modern medical billing, combined with ongoing regulatory updates and payer requirement changes, makes it increasingly difficult for practices to manage revenue cycles internally. These factors have accelerated adoption of specialized revenue cycle management solutions across organizations of all sizes.
Market Drivers Shaping Industry Growth
Several fundamental factors propel expansion within the revenue cycle management industry:
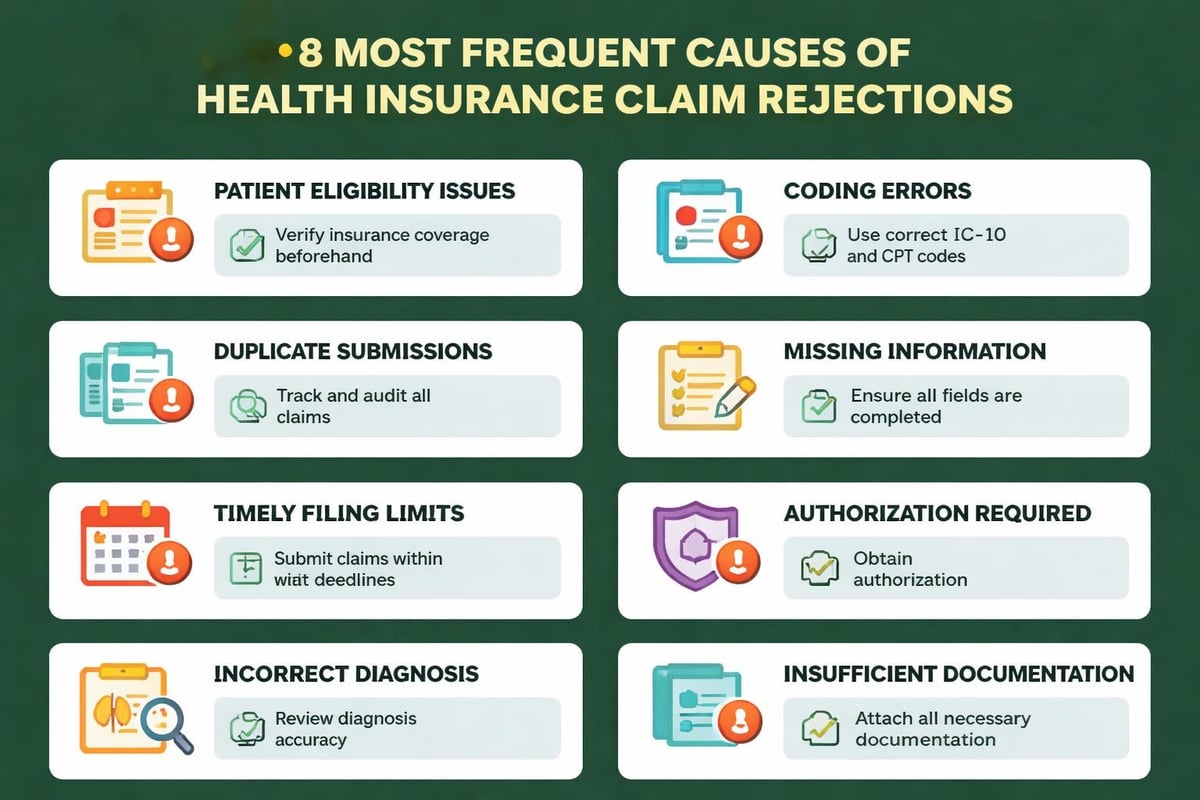
- Regulatory complexity: Frequent updates to coding requirements, compliance standards, and documentation rules
- Reimbursement pressures: Declining reimbursement rates and shift toward value-based payment models
- Administrative costs: Rising overhead expenses associated with maintaining in-house billing departments
- Technology requirements: Significant investment needed for software systems, updates, and staff training
- Staffing challenges: Difficulty recruiting and retaining qualified billing and coding professionals
The convergence of these pressures creates compelling reasons for healthcare organizations to evaluate external partnerships for their revenue cycle operations.
The Outsourcing Revolution in Revenue Cycle Management
Outsourcing has emerged as a dominant trend within the revenue cycle management industry, fundamentally changing how healthcare providers approach their financial operations. Market analysis of healthcare RCM outsourcing reveals consistent growth in organizations partnering with specialized service providers rather than maintaining entirely internal billing departments.
This shift reflects pragmatic business decisions rather than simple cost reduction strategies. Healthcare providers increasingly recognize that revenue cycle management requires specialized expertise, dedicated resources, and ongoing investment in technology and training. By partnering with experienced service providers, practices can access enterprise-level capabilities without the capital expenditure and management overhead required to build these competencies internally.
Benefits of Strategic Outsourcing Partnerships
Organizations that transition to outsourced revenue cycle management typically realize multiple advantages:
| Benefit Category | Impact on Practice Operations |
|---|---|
| Financial Performance | Improved collection rates, reduced days in A/R, increased clean claim rates |
| Operational Efficiency | Reduced administrative burden, freed staff capacity for patient care |
| Compliance Management | Maintained adherence to coding updates, payer requirements, regulatory changes |
| Technology Access | Utilization of advanced billing systems without direct investment |
| Scalability | Flexible capacity adjustment based on practice volume fluctuations |
Service providers within the revenue cycle management industry invest heavily in staff training, technology infrastructure, and process optimization. These investments benefit multiple clients simultaneously, creating economies of scale that individual practices cannot achieve independently.
Professional RCM partners bring specialized knowledge across diverse specialties and payer types. This breadth of experience proves particularly valuable when practices face denials, navigate complex prior authorization requirements, or address unusual billing scenarios. Teams that process thousands of claims daily develop pattern recognition and problem-solving capabilities that occasional processors simply cannot match.
Technology Integration and Innovation
The revenue cycle management industry has embraced technological advancement as a core driver of service quality and efficiency. While some healthcare providers invest directly in sophisticated billing software, many find greater value in partnering with service providers who utilize industry-standard platforms on their behalf.
This approach delivers several strategic advantages. Practices avoid the capital expense and ongoing licensing costs associated with premium billing systems. They eliminate the burden of software updates, maintenance, and troubleshooting. Perhaps most importantly, they gain access to teams with deep expertise in maximizing the capabilities of these platforms.
Essential Technology Components in Modern RCM
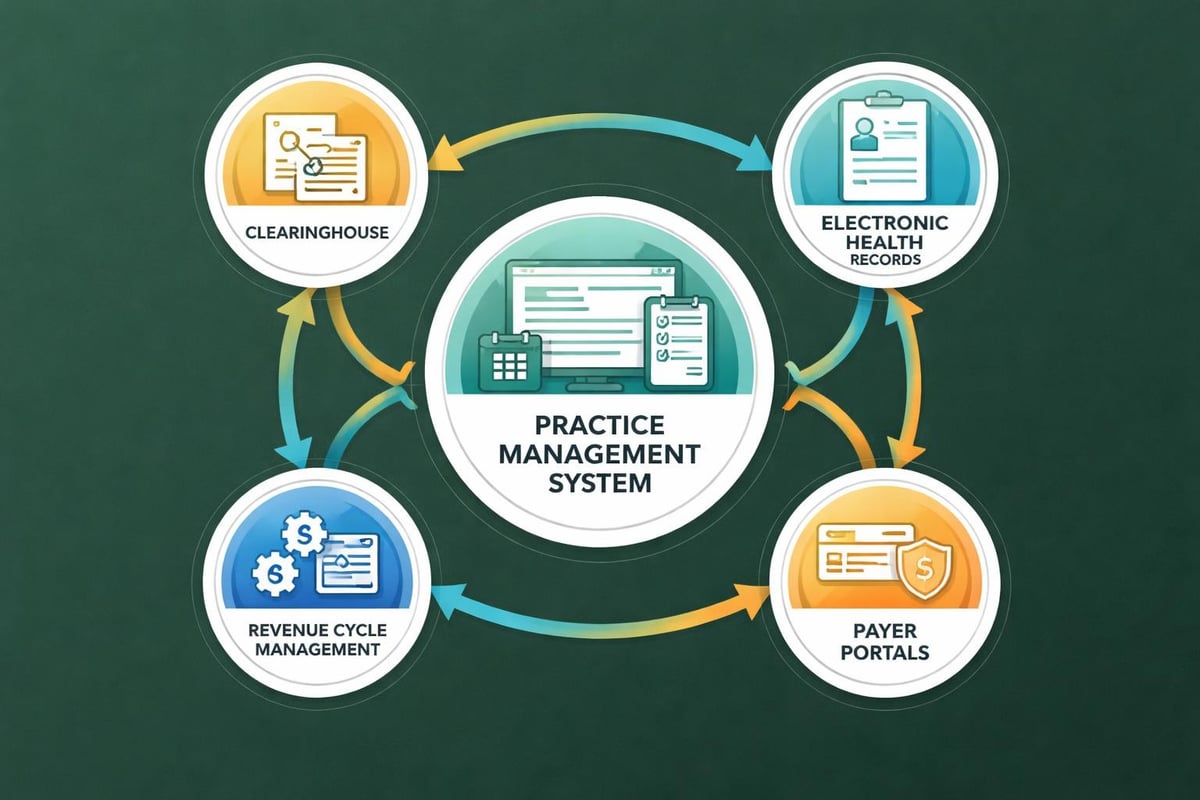
Contemporary revenue cycle management incorporates multiple technology layers that work together to optimize financial performance:
-
Electronic Health Records Integration: Seamless data flow between clinical documentation and billing systems ensures accurate charge capture and reduces manual data entry errors.
-
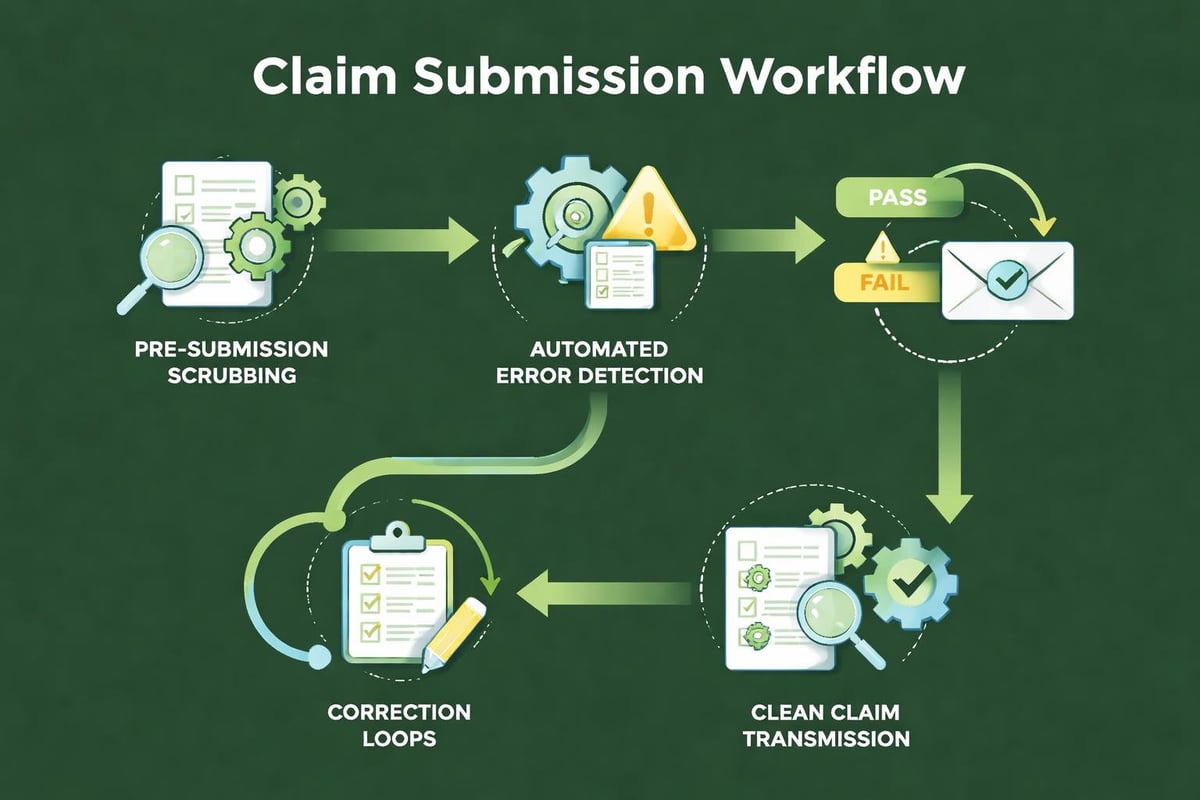
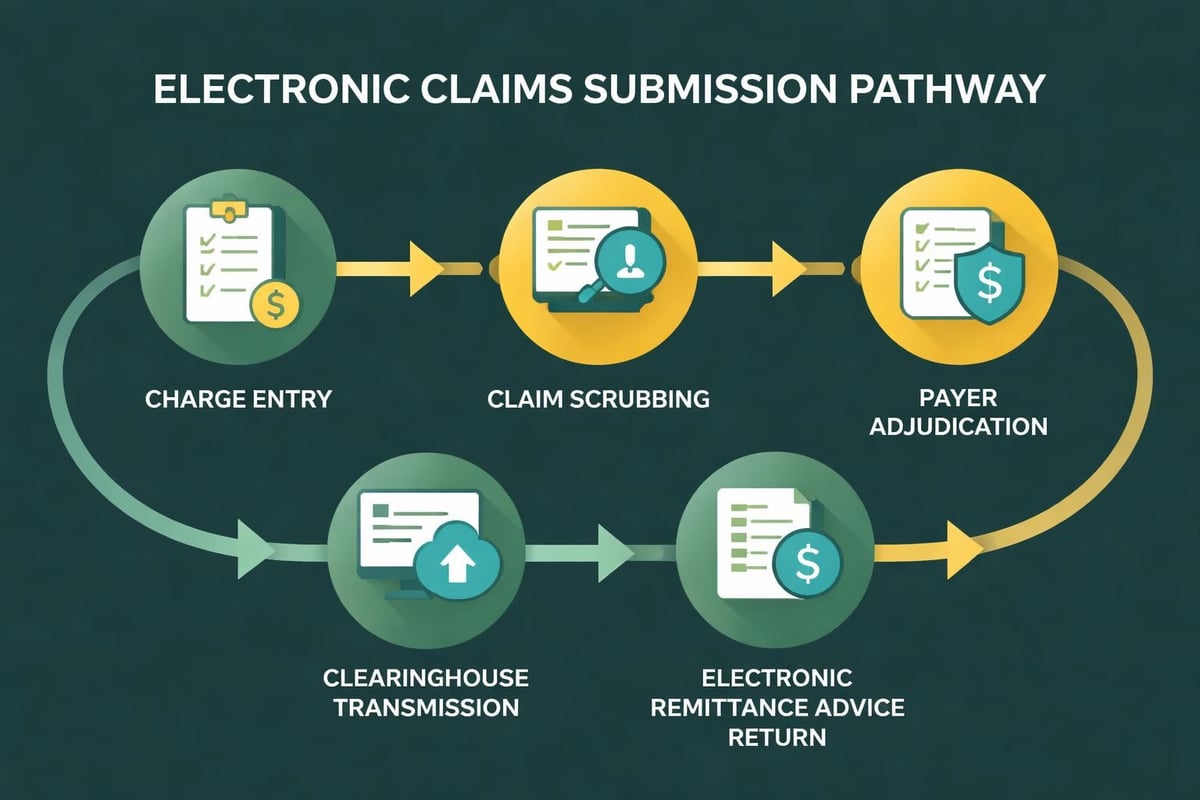
Claims Scrubbing Systems: Automated validation identifies potential rejections before claims reach payers, dramatically improving first-pass acceptance rates.
-
Eligibility Verification Tools: Real-time insurance verification reduces claim denials related to coverage issues and improves patient financial counseling.
-
Payment Posting Automation: Electronic remittance advice processing accelerates payment posting while reducing posting errors and improving reporting accuracy.
-
Denial Management Platforms: Systematic tracking and workflow management ensures timely appeal filing and identifies patterns requiring process correction.
Professional service providers invest in training their teams to use these tools effectively, adapting workflows to match client preferences while maintaining best practice standards. This combination of technology leverage and human expertise characterizes the modern revenue cycle management industry approach.
Understanding electronic remittance advice and its role in payment processing represents just one example of how technological literacy drives revenue cycle performance.
Denial Management as a Core Competency
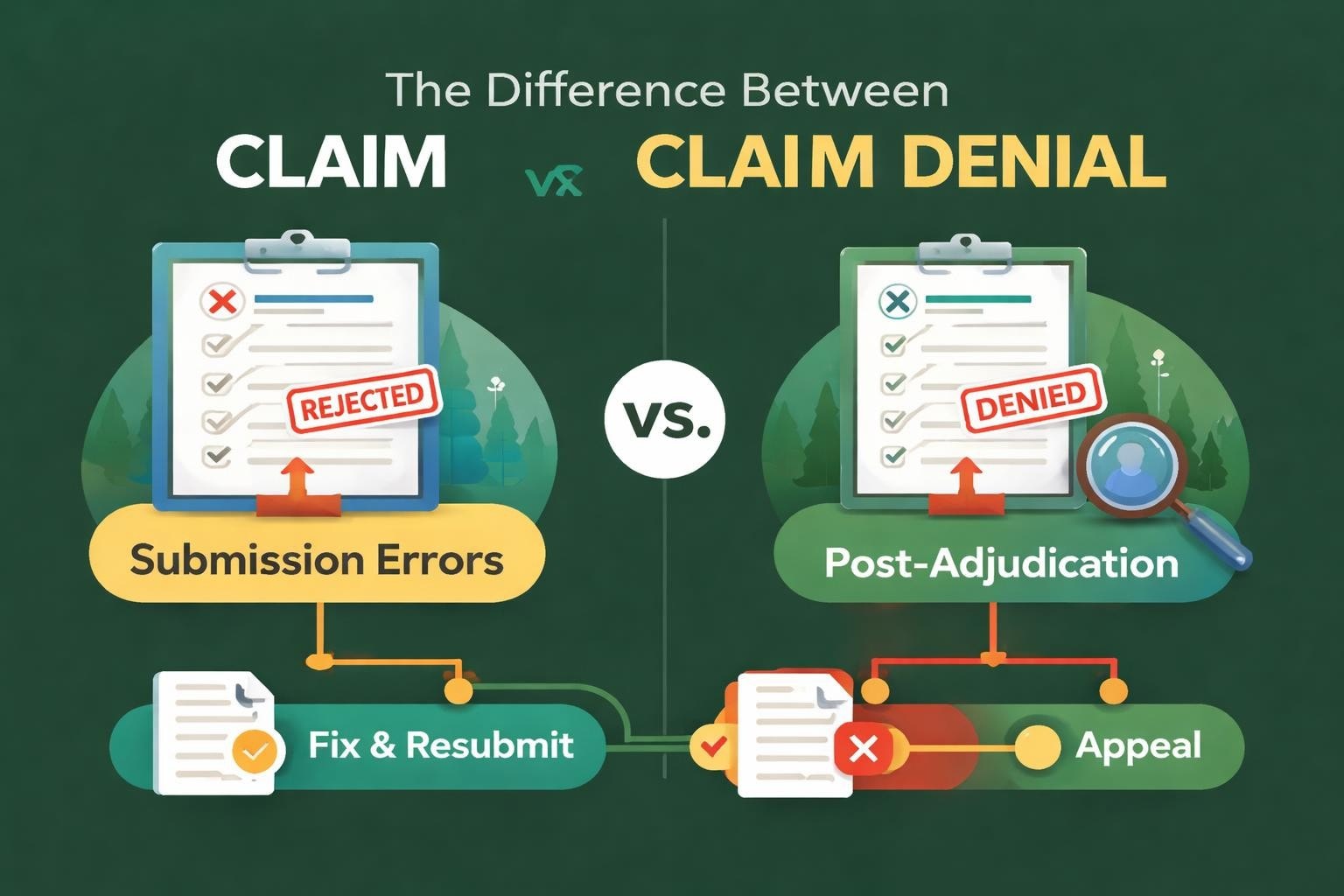
Claim denials represent one of the most significant challenges within healthcare revenue cycle operations, making denial management services a critical component of comprehensive RCM strategies. The revenue cycle management industry has developed sophisticated approaches to both preventing denials and efficiently resolving those that occur.
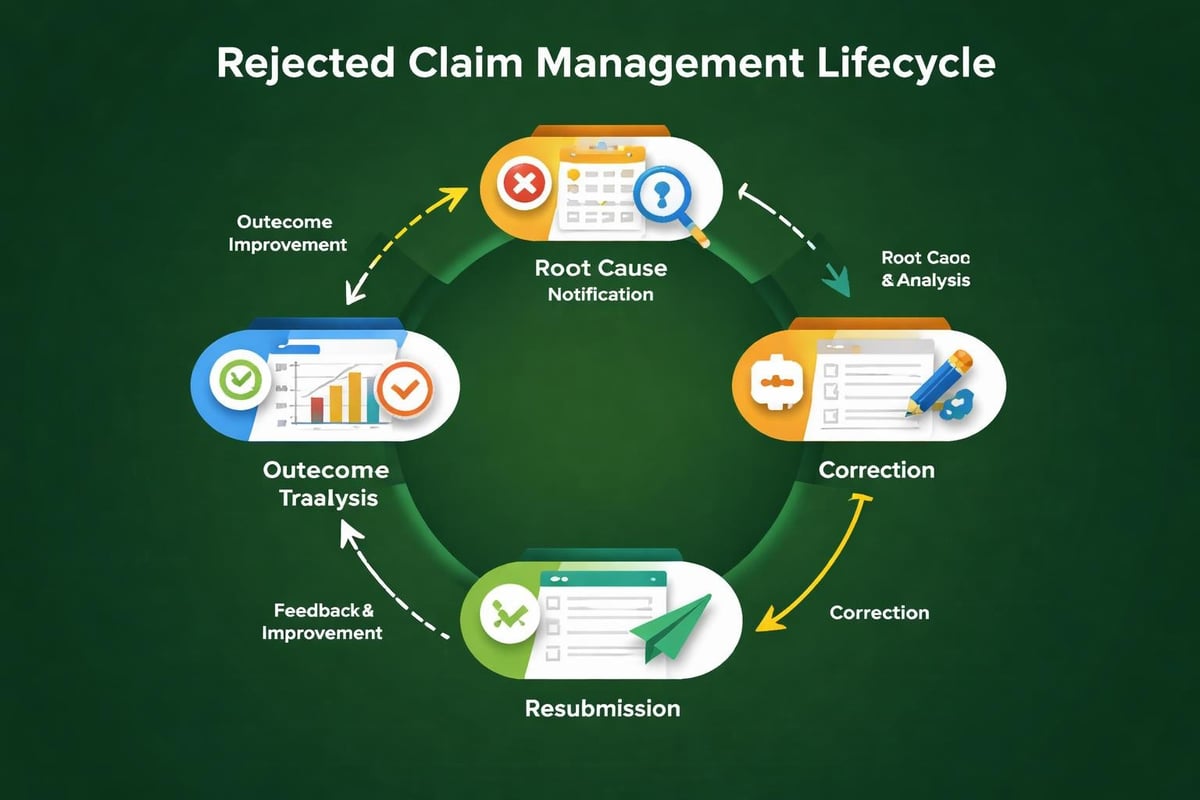
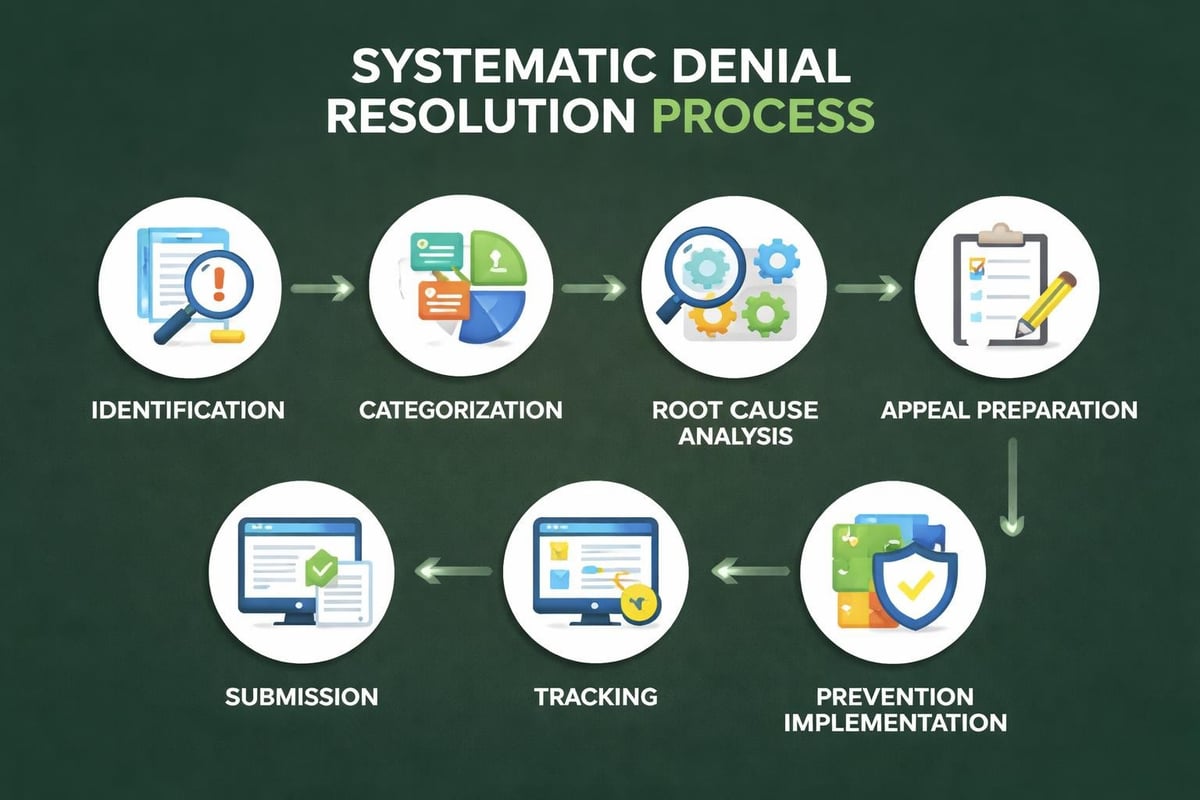
Effective denial management requires systematic processes, dedicated resources, and analytical capabilities that identify root causes rather than simply addressing symptoms. Organizations that excel in this area typically maintain detailed denial tracking, categorization systems, and performance metrics that guide continuous improvement efforts.
Strategic Denial Prevention and Resolution
Industry leaders approach denial management through multiple complementary strategies:
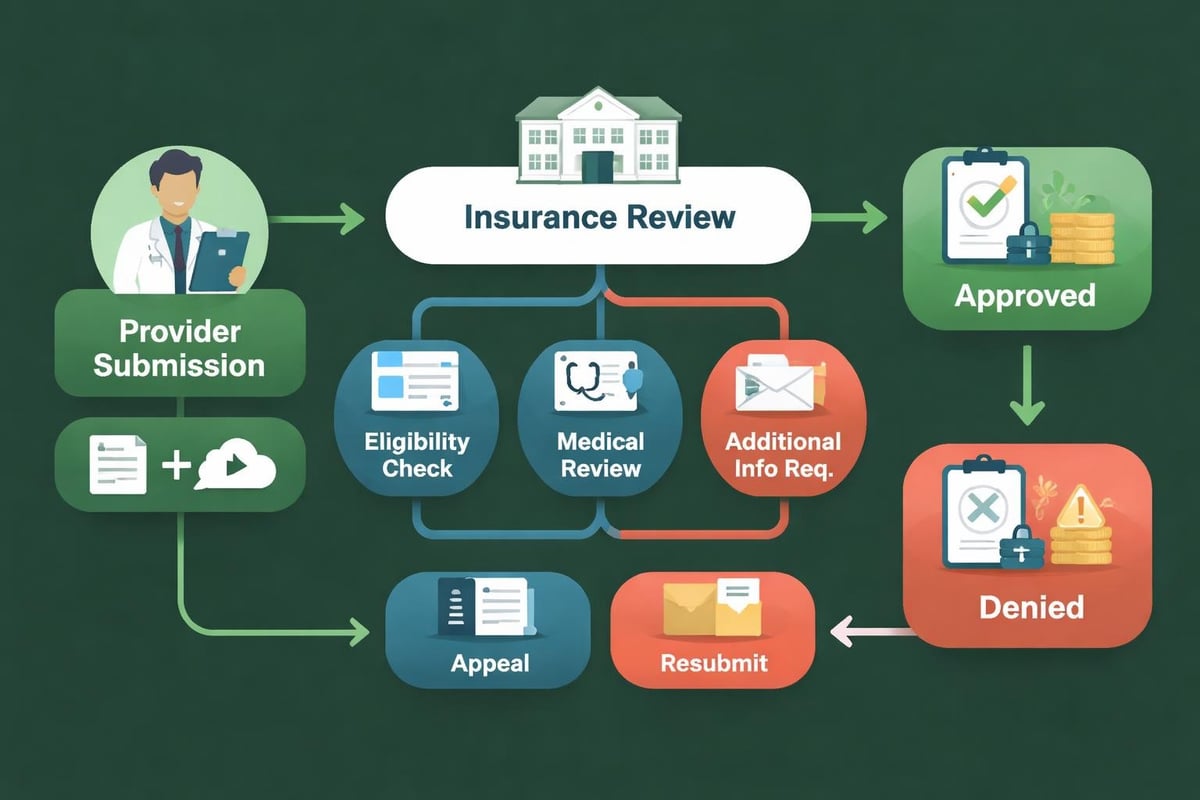
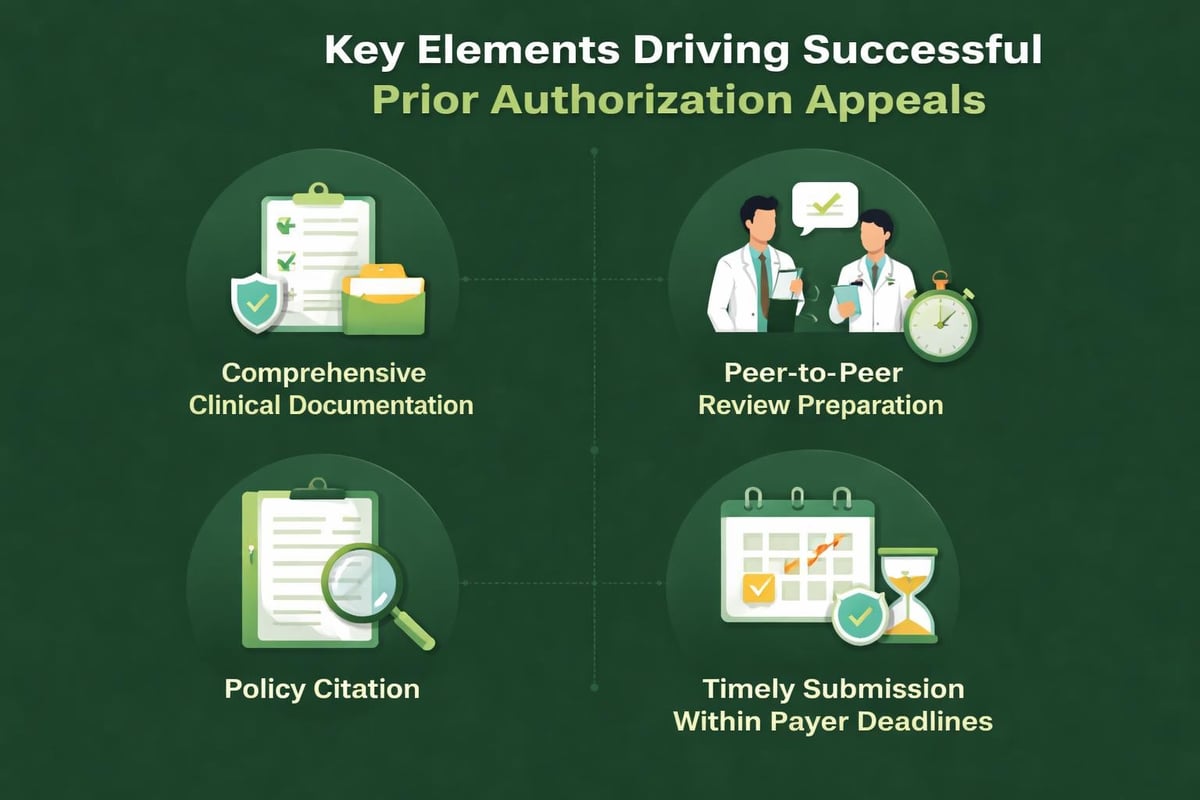
- Front-end prevention: Robust verification processes, accurate coding, and complete documentation before claim submission
- Timely appeals: Systematic workflow management ensures responses within payer deadlines
- Pattern analysis: Regular reporting identifies recurring issues requiring process or training corrections
- Payer communication: Established relationships facilitate quick resolution of ambiguous cases
- Documentation improvement: Feedback loops help clinical staff understand documentation requirements
The financial impact of effective denial management extends beyond recovered revenue. Practices that minimize denials reduce the administrative cost of rework, improve cash flow predictability, and maintain better relationships with both payers and patients.
Research from healthcare financial management associations consistently demonstrates that systematic denial management delivers measurable return on investment, making it a priority area for revenue cycle optimization.
Specialty-Specific Considerations
The revenue cycle management industry recognizes that different medical specialties face unique billing challenges, payer requirements, and documentation standards. Successful RCM strategies account for these variations, applying specialized knowledge rather than generic approaches.
Cardiology practices, for example, navigate complex procedure coding, significant prior authorization requirements, and high-dollar claims that demand meticulous documentation. Specialized cardiology billing expertise becomes essential for maximizing reimbursement while maintaining compliance.
Similarly, surgical specialties face modifier usage complexities, global period considerations, and assistant surgeon billing nuances that require specific training. Primary care practices, while often dealing with lower-dollar claims, process high volumes and must efficiently manage preventive service coding, chronic care management, and wellness visit documentation.
Adapting RCM Approaches by Practice Type
| Practice Type | Key Revenue Cycle Challenges | Specialized Requirements |
|---|---|---|
| Primary Care | High volume, preventive services, chronic care management | Efficient processing, wellness visit expertise, quality reporting |
| Surgical Specialties | Complex procedures, modifiers, global periods | Surgical coding expertise, modifier proficiency, documentation review |
| Diagnostic Services | Technical/professional splits, prior authorization | Authorization management, component billing, equipment validation |
| Mental Health | Session documentation, medical necessity | Privacy considerations, limited payer panels, documentation standards |
Organizations seeking revenue cycle management partners should prioritize those with demonstrated experience in their specific specialty. Generic billing knowledge provides insufficient foundation for navigating specialty-specific nuances that directly impact reimbursement.
Compliance and Regulatory Navigation
The revenue cycle management industry operates within an intensely regulated environment where compliance failures carry significant financial and legal consequences. Healthcare providers must maintain adherence to HIPAA privacy requirements, fraud and abuse regulations, coding guidelines, and payer-specific policies.
Professional RCM service providers assume responsibility for maintaining current knowledge of regulatory requirements and implementing compliant processes across their client base. This shared responsibility model reduces individual practice risk while ensuring consistent application of current standards.
Essential Compliance Domains in Revenue Cycle Management
Comprehensive compliance programs address multiple regulatory dimensions:
-
HIPAA Privacy and Security: Proper handling of protected health information throughout the revenue cycle, including secure transmission, access controls, and breach prevention protocols.
-
Coding Accuracy: Adherence to CPT, ICD-10, and HCPCS coding guidelines, including appropriate modifier usage and medical necessity support.
-
Billing Integrity: Honest and accurate claim submission, appropriate unbundling decisions, and proper use of revenue codes and place of service indicators.
-
Documentation Standards: Ensuring clinical documentation supports billed services and meets payer requirements for medical necessity and level of service.
-
Regulatory Reporting: Timely and accurate submission of quality measures, meaningful use attestations, and other regulatory reports impacting reimbursement.
The complexity and frequency of regulatory updates make ongoing education and process refinement essential. Organizations within the revenue cycle management industry invest substantially in compliance training, audit programs, and policy updates to protect both their operations and their clients' interests.

Market Consolidation and Strategic Partnerships
The revenue cycle management industry has experienced notable consolidation activity, with mergers and acquisitions reshaping competitive dynamics. Larger organizations acquire specialized providers to expand service capabilities, geographic reach, or technology platforms, creating more comprehensive service offerings.
This consolidation trend reflects market maturation and recognition that scale provides competitive advantages in technology investment, staff development, and operational efficiency. However, consolidation also creates opportunities for focused specialists who deliver exceptional service in specific niches or geographic markets.
Healthcare providers evaluating potential RCM partners should consider both the stability that larger organizations provide and the personalized attention that smaller, focused providers often deliver. The optimal choice depends on practice size, specialty, geographic location, and specific service requirements.
Evaluating Revenue Cycle Management Partners
When selecting external revenue cycle management support, healthcare organizations should assess multiple dimensions:
- Industry experience: Years in business, client retention rates, and references from similar practices
- Specialty expertise: Demonstrated knowledge of specific medical specialties and their unique requirements
- Technology capabilities: Platforms utilized, reporting capabilities, and integration with existing practice systems
- Service model: Dedicated teams versus shared resources, communication protocols, and escalation procedures
- Performance metrics: Transparent reporting on key indicators like clean claim rates, days in A/R, and collection percentages
- Compliance programs: Audit processes, staff training, and regulatory update procedures
Organizations seeking top medical billing companies should conduct thorough due diligence, checking references and requesting detailed information about processes, technology, and performance guarantees.
Financial Performance Metrics and Benchmarking
The revenue cycle management industry has developed standardized metrics that enable healthcare organizations to assess performance objectively and identify improvement opportunities. Understanding and tracking these key performance indicators provides essential visibility into revenue cycle health.
Professional RCM service providers typically offer comprehensive reporting that tracks performance across multiple dimensions, enabling practices to monitor trends, identify issues early, and make data-driven decisions about resource allocation and process improvements.
Critical Revenue Cycle Performance Indicators
| Metric | Definition | Industry Benchmark |
|---|---|---|
| Clean Claim Rate | Percentage of claims accepted without edits on first submission | 95% or higher |
| Days in A/R | Average days from service date to payment receipt | 30-40 days |
| Collection Rate | Net collections as percentage of adjusted charges | 95% or higher |
| Denial Rate | Percentage of submitted claims initially denied | 5% or lower |
| Cost to Collect | Administrative cost per dollar collected | 3-5% of collections |
Regular performance review enables practices to identify trends before they significantly impact cash flow. For example, gradual increases in denial rates might indicate coding changes, payer policy updates, or documentation issues requiring attention.
Benchmarking against industry standards provides context for performance assessment. While every practice faces unique circumstances, significant variance from benchmarks typically signals opportunities for improvement or underlying issues requiring investigation.
Future Trends Shaping the Revenue Cycle Management Industry
The revenue cycle management industry continues evolving in response to healthcare delivery changes, technological advancement, and regulatory developments. Organizations planning long-term RCM strategies should consider emerging trends likely to shape the landscape in coming years.
Artificial intelligence and machine learning increasingly enhance revenue cycle processes, from predictive analytics that identify likely denials to natural language processing that extracts billable elements from clinical documentation. While these technologies supplement rather than replace human expertise, they enable more efficient operations and more strategic resource allocation.
Emerging Developments in Revenue Cycle Operations
Forward-looking organizations monitor several key trend areas:
-
Value-Based Reimbursement: Continued shift from fee-for-service toward quality-based payment models requires new reporting capabilities and performance tracking.
-
Patient Financial Responsibility: Growing deductibles and copayments increase the importance of front-end collections and patient financing options.
-
Interoperability Requirements: Information blocking rules and standardized data exchange protocols facilitate better coordination across care teams and payers.
-
Automation Expansion: Robotic process automation handles repetitive tasks, freeing staff for complex problem-solving and patient interaction.
-
Predictive Analytics: Advanced reporting identifies patterns and trends that enable proactive intervention before issues impact revenue.
Healthcare organizations partnering with experienced revenue cycle management service providers gain access to these innovations without direct investment, benefiting from industry-wide advancement while maintaining focus on clinical excellence.
Choosing Between In-House and Outsourced Models
Healthcare providers frequently evaluate whether to maintain in-house revenue cycle operations, fully outsource these functions, or adopt hybrid approaches that combine internal and external resources. The revenue cycle management industry offers flexible engagement models that accommodate different organizational preferences and requirements.
Fully in-house operations provide maximum control and direct staff oversight but require significant investment in recruitment, training, technology, and ongoing management. Organizations choosing this path must commit to continuous staff development, regular technology updates, and dedicated leadership focus on revenue cycle performance.
Complete outsourcing transfers responsibility for revenue cycle operations to specialized service providers, enabling practices to redirect internal resources toward patient care and clinical operations. This model works particularly well for small practices that lack the scale to maintain specialized billing departments efficiently.
Hybrid Revenue Cycle Management Approaches
Many organizations find optimal results through hybrid models that leverage both internal and external resources:
- Front-end internal, back-end external: Practice staff handle registration, verification, and charge entry while external partners manage claims submission, payment posting, and follow-up
- Specialty-specific outsourcing: Routine claims processed internally with complex or specialty-specific billing handled by experts
- Overflow support: External partners provide surge capacity during high-volume periods or staff shortages
- Project-based engagement: Specialists address specific challenges like denial backlogs or payer audits
The optimal model depends on practice size, specialty, staff capabilities, technology infrastructure, and strategic priorities. Regular reassessment ensures the chosen approach continues meeting evolving needs.
Regional Considerations and Local Expertise
While many aspects of revenue cycle management apply universally, regional variations in payer mix, regulatory requirements, and market dynamics influence optimal strategies. The revenue cycle management industry includes both national providers serving clients across multiple states and regional specialists with deep local market knowledge.
Practices operating in specific geographic markets often benefit from partners familiar with dominant local payers, state-specific Medicaid programs, and regional regulatory requirements. For example, Arizona medical billing expertise provides value for practices in that state navigating AHCCCS requirements and local commercial payer policies.
Similarly, practices in major metropolitan areas face unique payer landscapes and competitive dynamics that influence revenue cycle strategies. California healthcare providers navigate Medi-Cal managed care plans, while those in major cities like Los Angeles deal with diverse payer mixes and high patient volumes.
Geographic Factors Influencing RCM Strategy
Regional characteristics affecting revenue cycle performance include:
- Payer mix: Dominant insurance carriers, Medicaid managed care penetration, Medicare Advantage prevalence
- State regulations: State-specific coding requirements, billing regulations, and licensing standards
- Market competition: Provider density, payer negotiating dynamics, and patient access patterns
- Economic factors: Uninsured rates, median incomes, and employer coverage patterns
- Technology adoption: Regional variations in EHR platforms, clearinghouse preferences, and payer portal capabilities
Revenue cycle management partners with broad geographic experience can identify best practices from diverse markets while applying specific knowledge of local requirements and payer behaviors.
Service Integration and Comprehensive Solutions
The revenue cycle management industry increasingly offers comprehensive service packages that address multiple aspects of healthcare financial operations. Rather than engaging separate vendors for eligibility verification, claims submission, payment posting, and prior authorization, practices can partner with providers offering integrated solutions.
This integrated approach delivers several advantages over fragmented vendor relationships. Single-source accountability eliminates finger-pointing when issues arise. Unified data flows reduce duplicate entry and integration challenges. Consistent processes across revenue cycle stages improve efficiency and reduce errors.
Comprehensive service providers typically offer:
- Front-end services: Patient scheduling support, insurance verification, authorization management
- Charge capture: Coding review, charge entry, compliance verification
- Claims management: Electronic submission, clearinghouse management, rejection resolution
- Payment processing: ERA posting, correspondence handling, adjustment review
- Follow-up services: Denial management, appeal filing, patient billing and collections
- Reporting and analytics: Performance dashboards, trend analysis, actionable insights
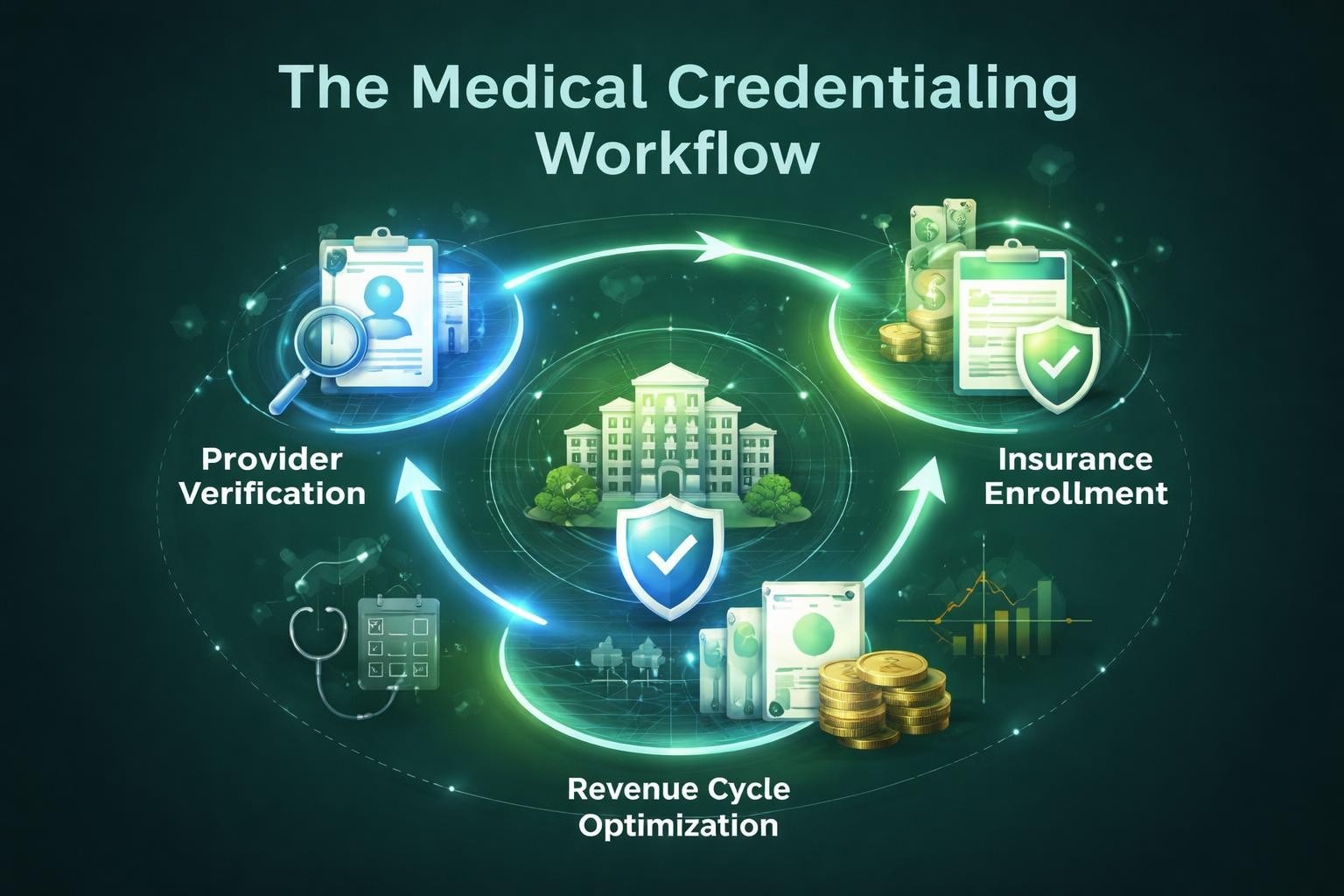
Integration with related services like medical credentialing and coding audit services creates even more comprehensive support that addresses interconnected aspects of healthcare financial management.
The revenue cycle management industry continues evolving to meet healthcare providers' changing needs, offering sophisticated solutions that improve financial performance while reducing administrative burden. Success in modern healthcare requires strategic approaches to revenue cycle operations, whether through internal excellence, external partnerships, or hybrid models that leverage the strengths of both.
Greenhive Billing Solutions delivers comprehensive revenue cycle management services specifically designed for healthcare providers seeking to optimize financial performance while maintaining focus on patient care. Our experienced team provides medical billing, eligibility verification, claims processing, and denial management services with HIPAA-compliant processes and transparent communication, helping practices across the United States achieve maximum reimbursements and operational efficiency.