Understanding revenue cycle processes is essential for healthcare providers seeking to maintain financial stability and operational efficiency. These processes encompass every step from patient registration through final payment collection, representing the financial backbone of medical practices. For healthcare organizations across the United States, mastering these workflows directly impacts cash flow, reduces claim denials, and ensures sustainable operations.
The Foundation of Revenue Cycle Processes
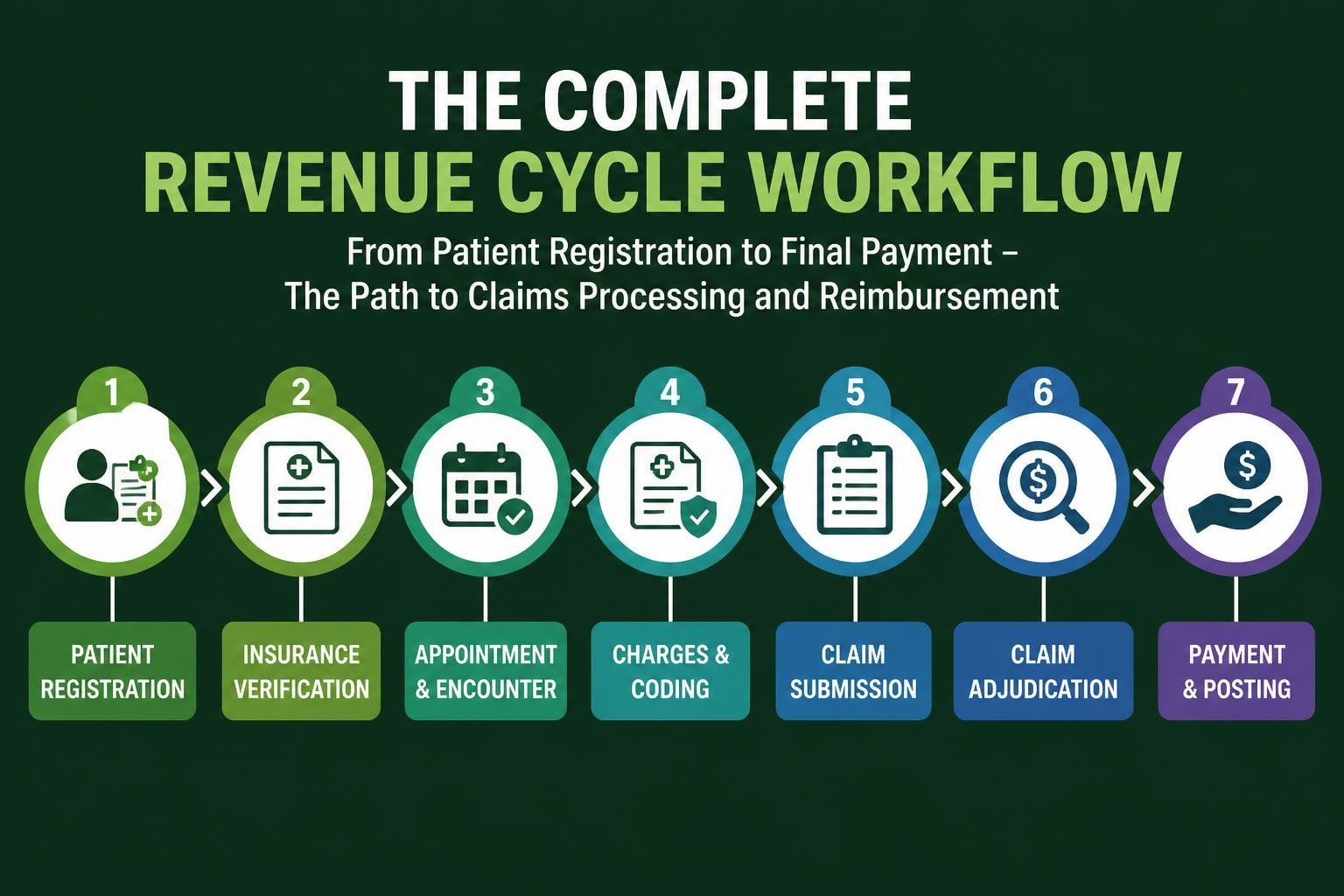
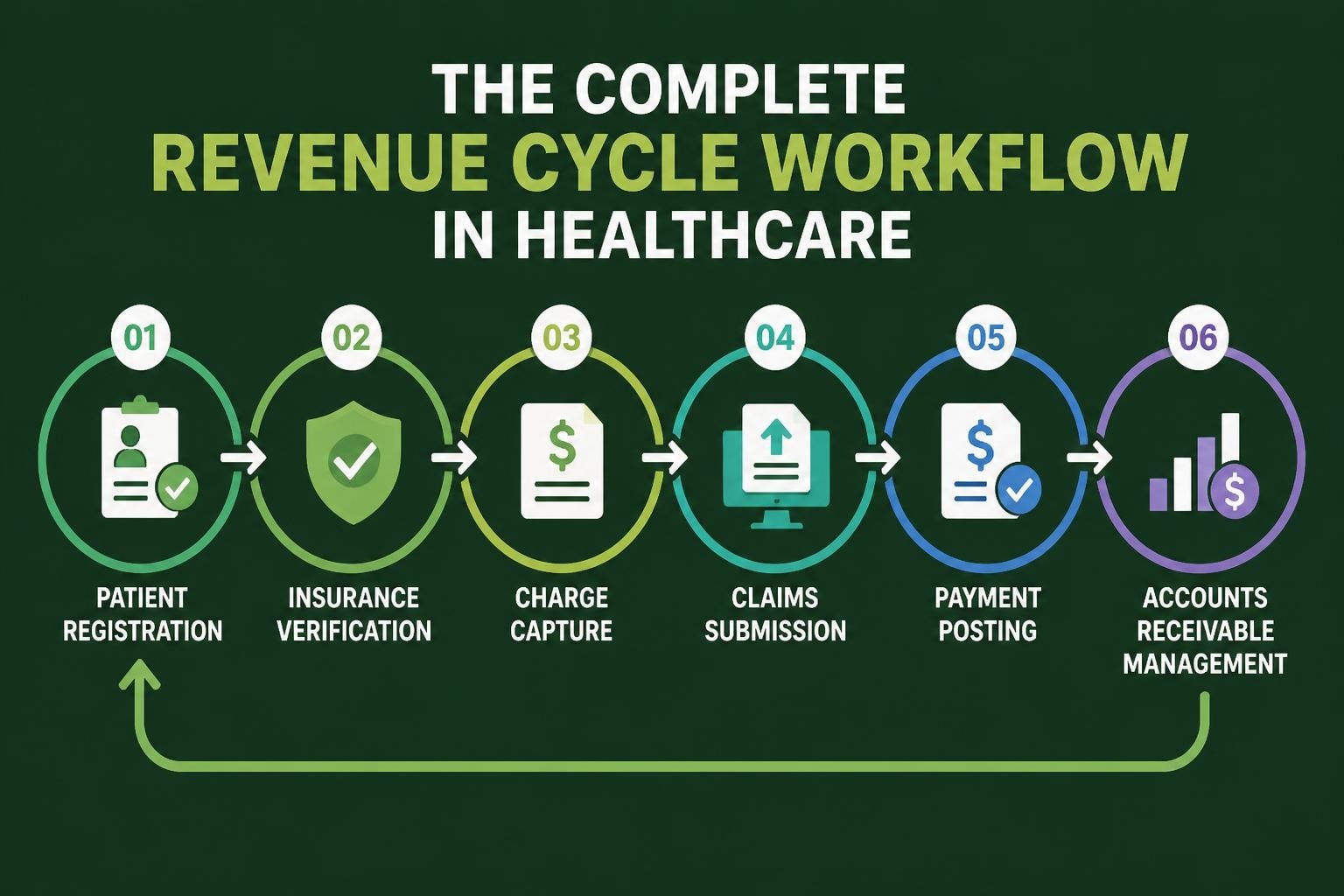
Revenue cycle processes begin long before a patient receives treatment and continue well after their visit concludes. According to the Healthcare Financial Management Association’s overview of revenue cycle management, these interconnected steps form a comprehensive system designed to track patient care episodes from initial contact through final payment reconciliation.
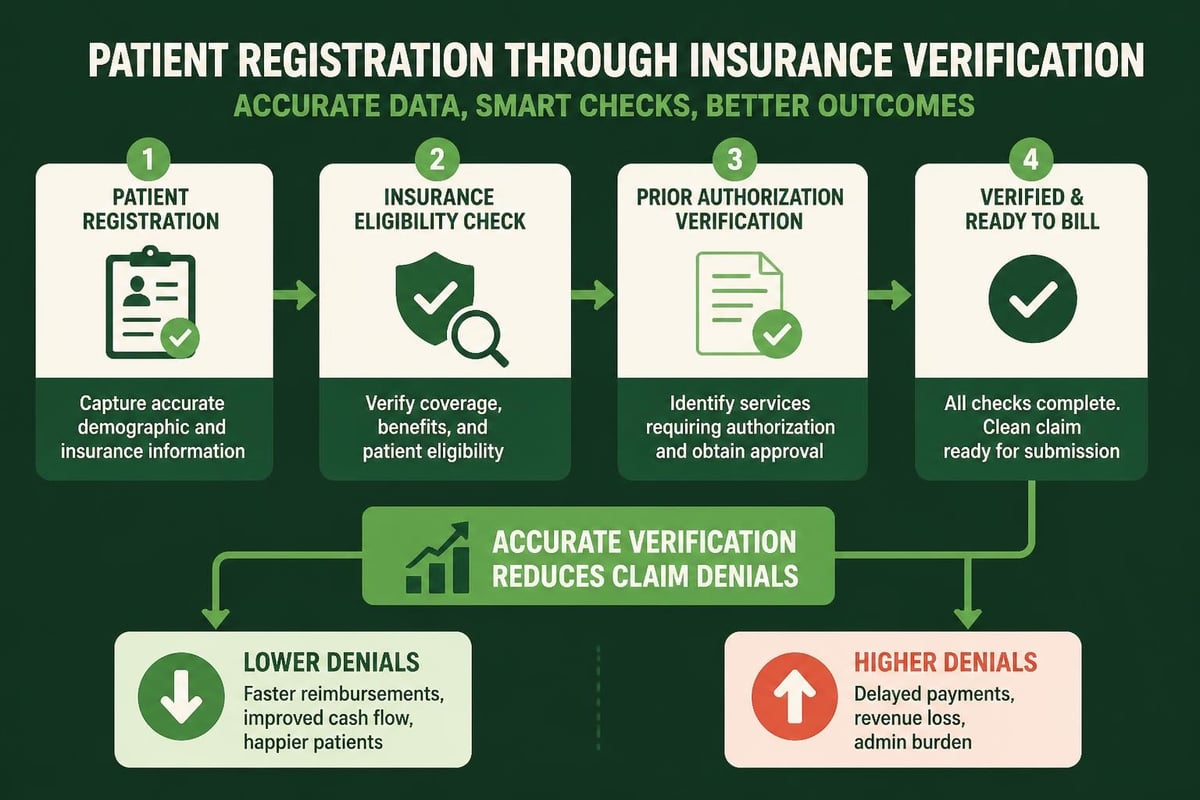
The front-end processes set the tone for everything that follows. Patient registration, insurance eligibility verification, and pre-authorization occur during this critical phase. When healthcare providers invest in thorough eligibility verification services, they significantly reduce the risk of claim denials and payment delays downstream.
Front-End Revenue Cycle Components
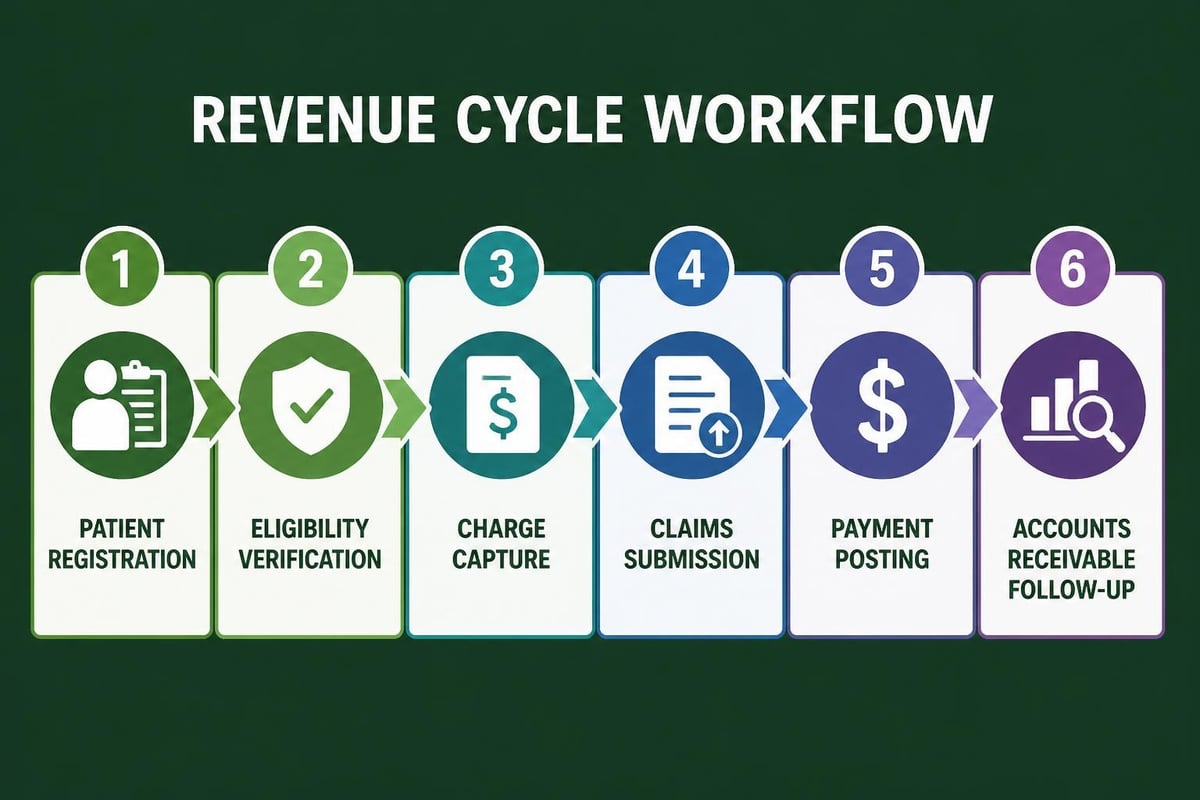
Front-end revenue cycle processes require meticulous attention to detail and accurate data collection. These initial steps include:
- Patient demographic capture with complete and accurate information
- Insurance verification to confirm coverage and benefits
- Prior authorization for procedures requiring payer approval
- Financial counseling to discuss patient responsibility and payment options
- Point-of-service collections for copays and deductibles
Each component serves as a building block for successful reimbursement. When registration staff collect incomplete or inaccurate information, the ripple effect impacts every subsequent stage of the revenue cycle.
Mid-Cycle Operations and Charge Capture
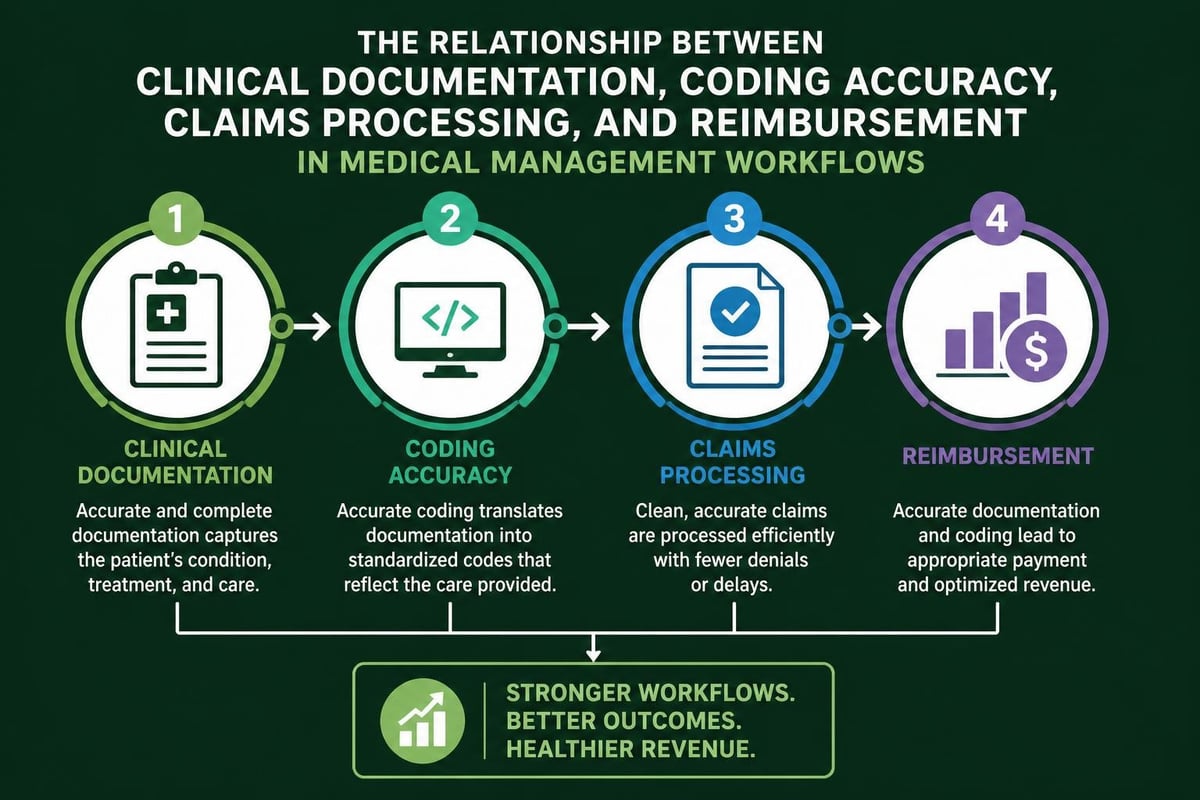
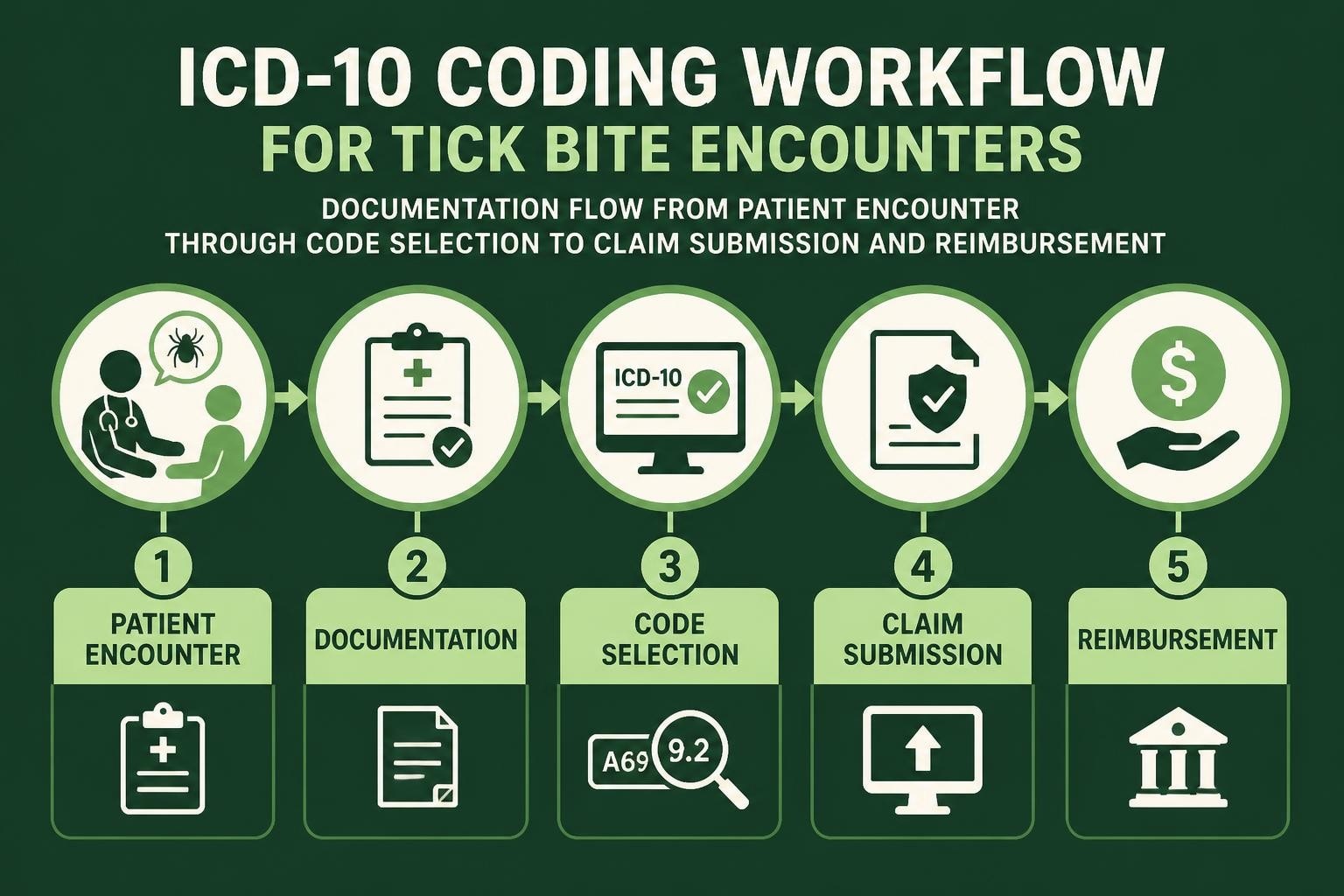
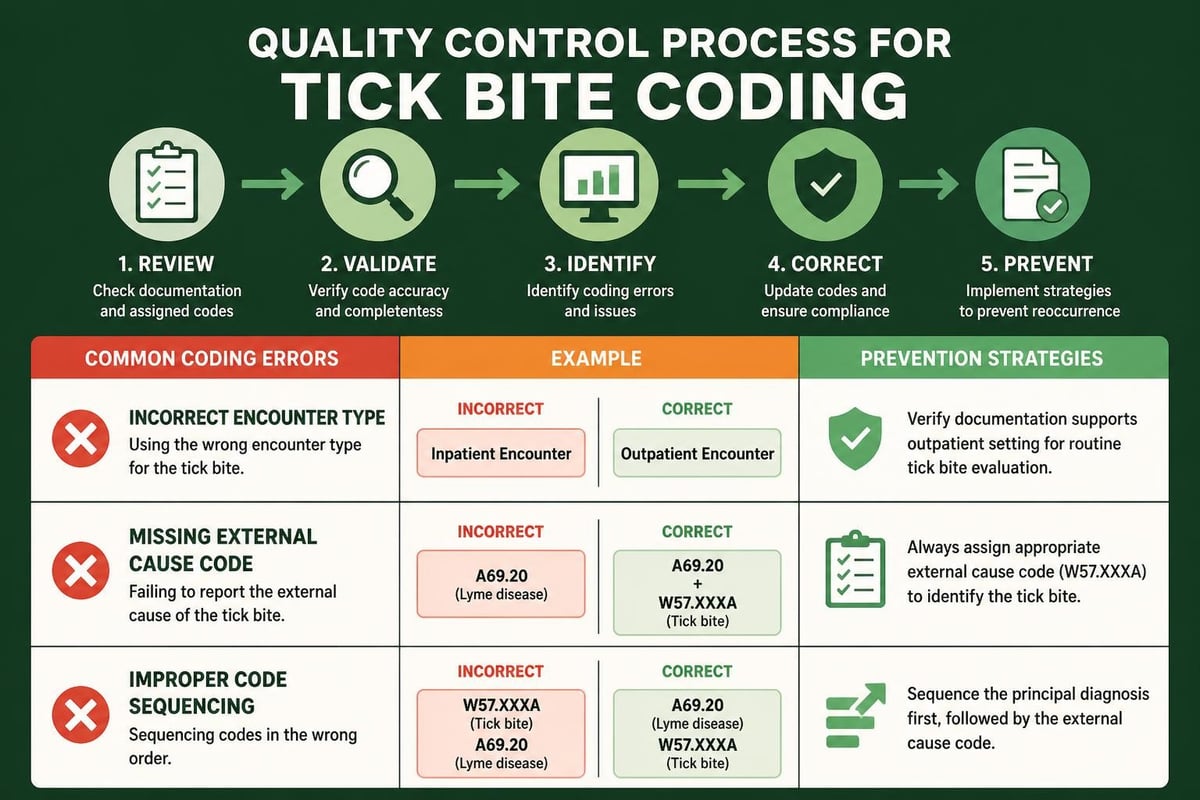
The middle phase of revenue cycle processes encompasses charge capture, medical coding, and claims submission. This stage transforms clinical documentation into billable claims that payers can process and reimburse.
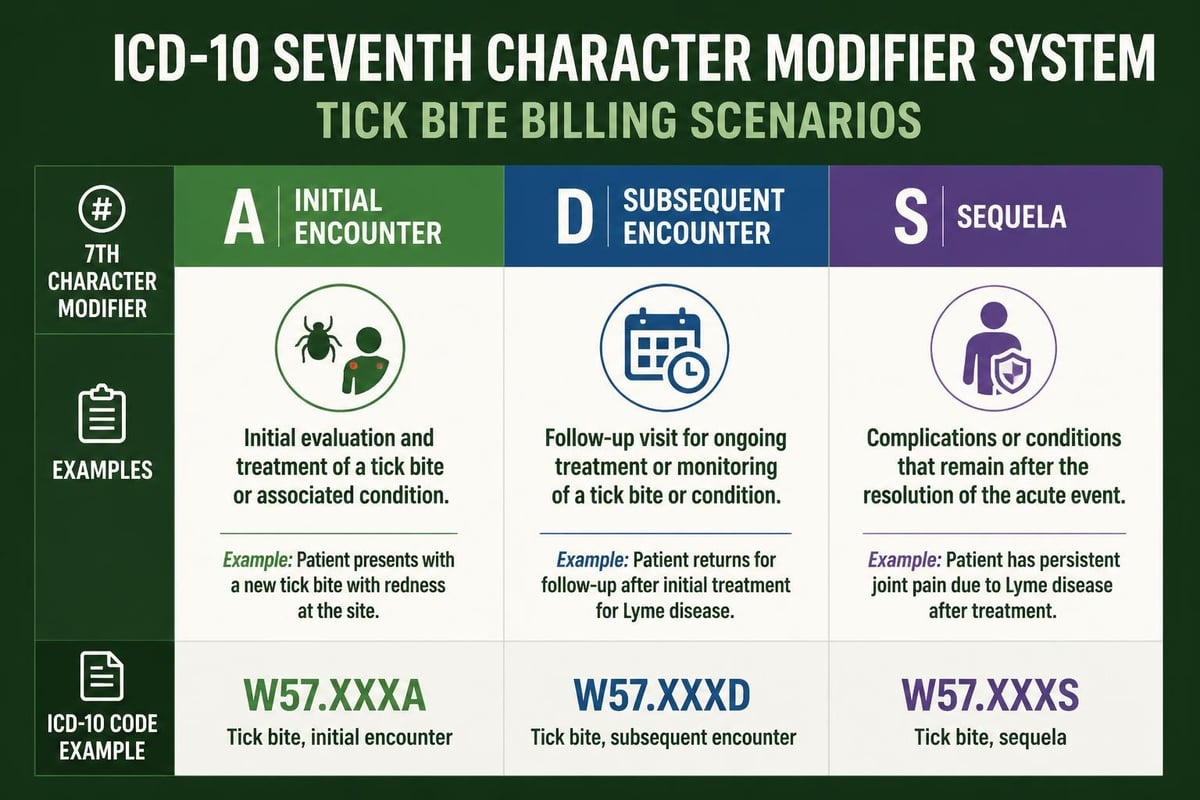
Charge capture requires systematic protocols to ensure all billable services receive appropriate documentation. Healthcare providers must bridge the gap between clinical care delivery and financial documentation. Medical coders then translate provider notes into standardized codes using ICD-10, CPT, and HCPCS code sets.
Claims Submission Excellence
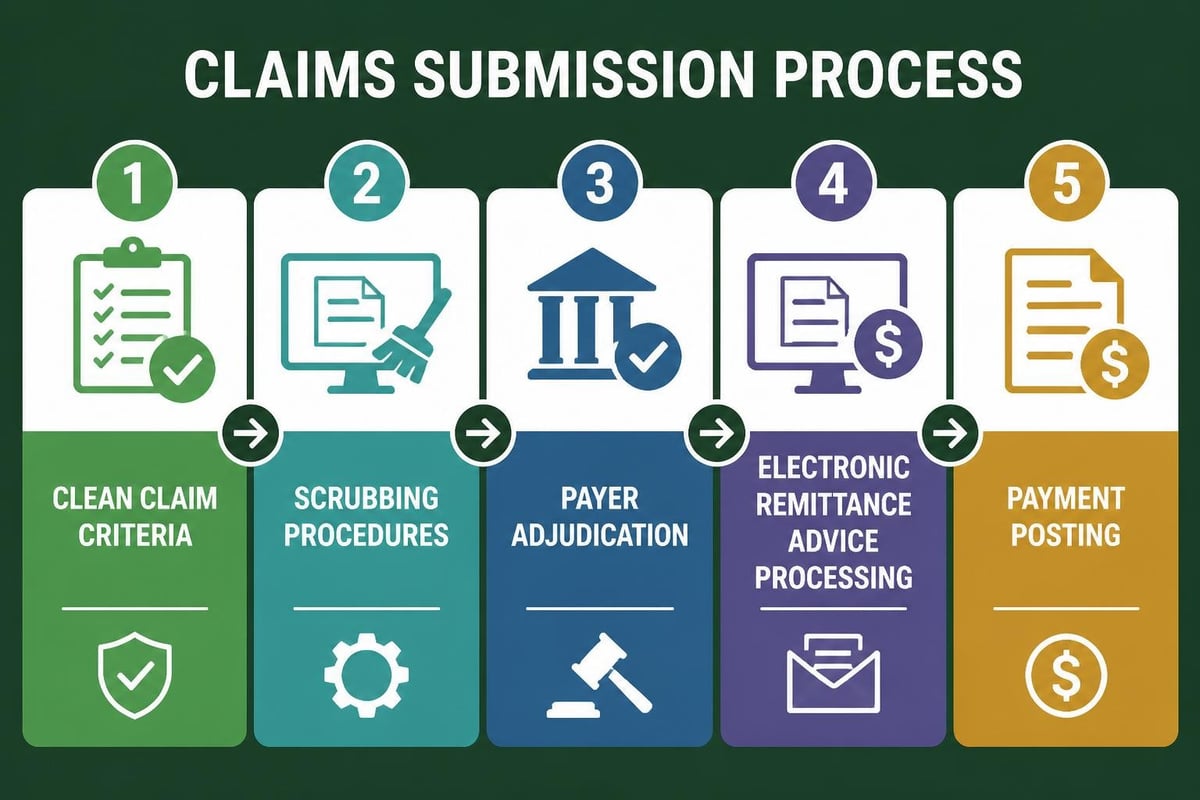
Professional medical claim submission services follow strict protocols to maximize clean claim rates. The submission process demands attention to multiple elements:
- Verification of code accuracy against current guidelines and payer requirements
- Review of documentation to support medical necessity
- Compliance checks for coding rules and modifier usage
- Scrubbing claims through automated edits before submission
- Electronic transmission to appropriate payers via clearinghouses
Claims scrubbing identifies errors before submission, preventing rejections and accelerating payment timelines. Research from TechTarget’s explanation of revenue cycle management indicates that clean claim rates directly correlate with improved days in accounts receivable.
| Revenue Cycle Stage | Key Activities | Success Metrics |
|---|---|---|
| Front-End | Registration, verification, authorization | Accuracy rate, pre-authorization approval rate |
| Mid-Cycle | Charge capture, coding, claims submission | Clean claim rate, submission timeliness |
| Back-End | Payment posting, denial management, A/R follow-up | Collection rate, denial rate, days in A/R |
Back-End Revenue Cycle Processes
Back-end revenue cycle processes focus on payment collection, denial resolution, and accounts receivable management. This phase determines how quickly and completely healthcare providers receive reimbursement for services rendered.
Payment posting must occur promptly and accurately to maintain current financial records. Staff members reconcile payments against billed amounts, identify underpayments, and flag discrepancies requiring investigation. Professional payment posting services ensure accurate allocation of payments across multiple patients and service lines.
Denial Management Strategies
Denial management represents a critical component of revenue cycle processes. According to TechTarget’s analysis of back-end revenue cycle practices, effective denial management requires systematic approaches to identify, appeal, and prevent claim denials.
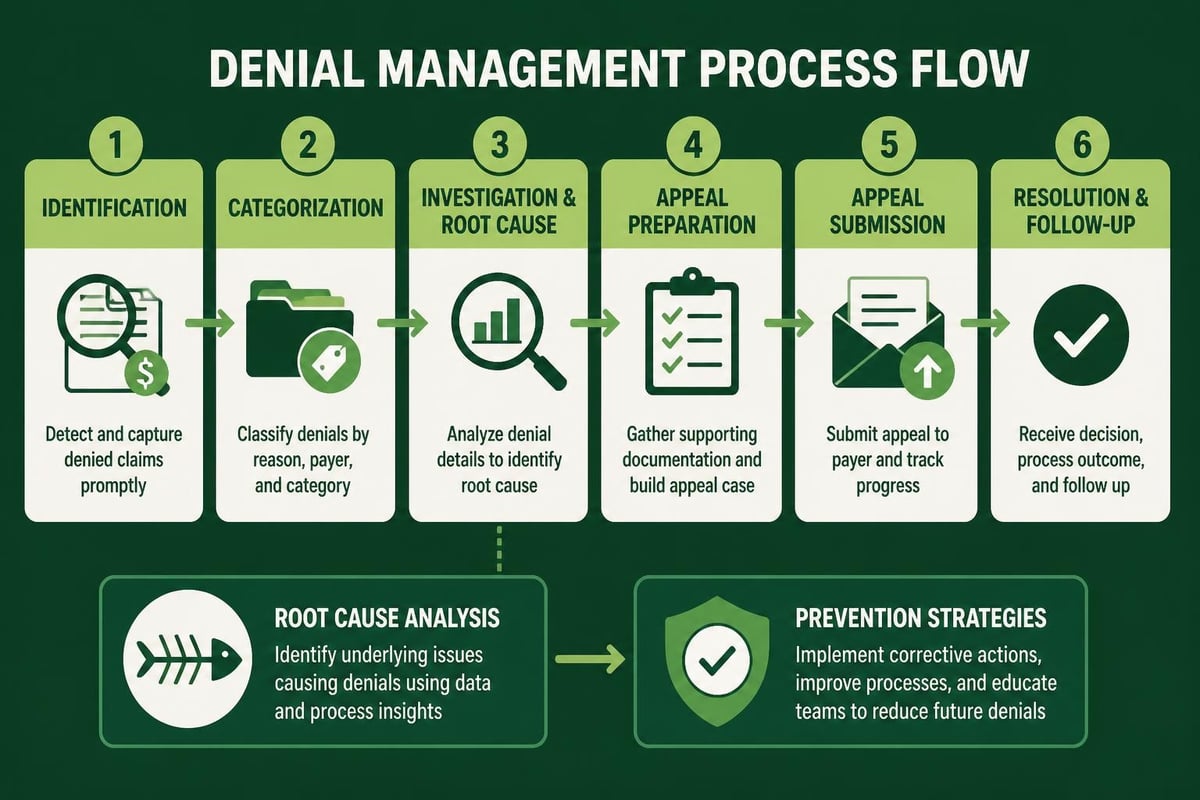
Healthcare providers benefit from implementing comprehensive denial management services that address both immediate appeals and root cause analysis. The denial management workflow includes:
- Prompt identification of denied claims through automated alerts
- Classification of denial reasons into categories for trending
- Timely appeals with supporting documentation
- Root cause analysis to prevent future denials
- Staff education based on denial patterns
Tracking denial patterns reveals opportunities for process improvement across all revenue cycle stages. When providers identify recurring issues with specific payers or procedure codes, they can implement targeted corrective actions.
Technology Integration in Revenue Cycle Processes
Modern revenue cycle processes rely heavily on technology solutions to improve efficiency and accuracy. Healthcare providers leverage revenue cycle technology that optimizes operations through automation, analytics, and integration capabilities.
Practice management systems, electronic health records, and specialized billing platforms work together to streamline workflows. Automation reduces manual data entry, minimizes human error, and accelerates claim processing timelines. Advanced analytics provide insights into performance metrics, helping administrators identify bottlenecks and opportunities for improvement.
Performance Monitoring and Analytics
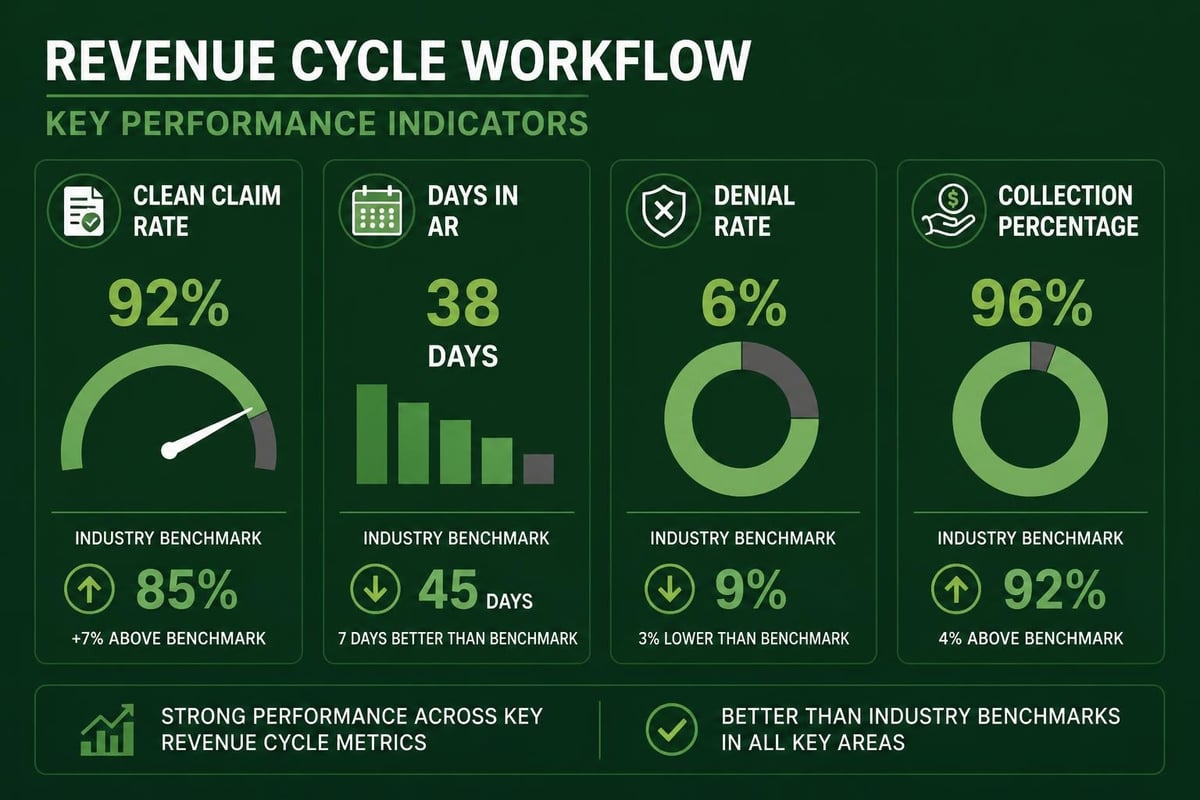
Healthcare organizations benefit from implementing healthcare revenue cycle analytics to track key performance indicators. The HFMA MAP Keys provide industry-standard benchmarks for measuring revenue cycle performance across multiple dimensions.
Critical metrics include:
- Days in accounts receivable
- Clean claim rate
- Net collection rate
- Cost to collect
- Point-of-service cash collections
- Denial rate by category
Regular monitoring of these indicators allows healthcare providers to identify trends before they impact cash flow significantly. Benchmarking against industry standards reveals areas where performance lags and opportunities exist for optimization.
Optimizing Revenue Cycle Processes for Maximum Efficiency
Successful revenue cycle processes require ongoing optimization and continuous improvement initiatives. Healthcare providers must balance efficiency with accuracy, compliance with productivity, and automation with human oversight.
Staff training plays a fundamental role in process optimization. When team members understand how their responsibilities connect to overall revenue cycle performance, they make better decisions and take ownership of outcomes. Cross-training creates flexibility and ensures continuity during staff transitions or volume fluctuations.
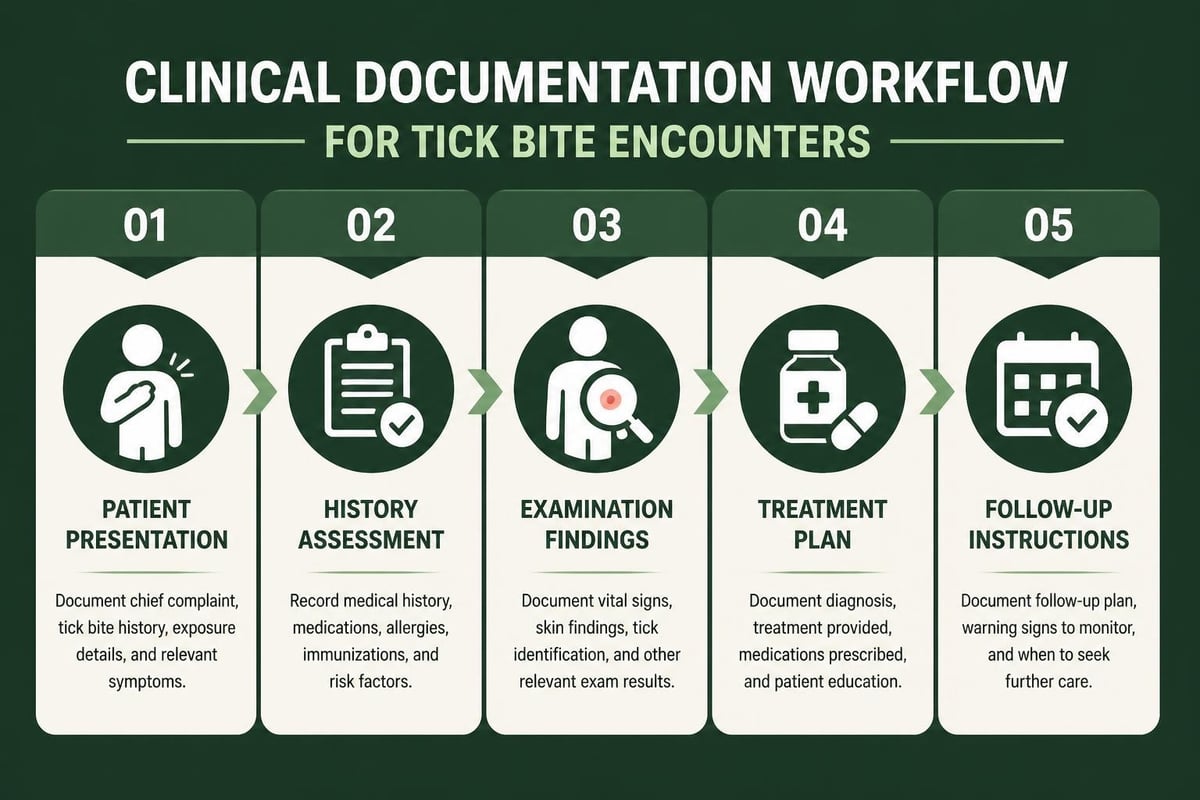
Documentation standards must align with coding requirements and payer expectations. Providers who invest in physician education about documentation quality see measurable improvements in code specificity, reimbursement accuracy, and reduced queries from coding staff.
Regular audits identify compliance risks and process gaps before they result in significant financial impact. Internal reviews of coding accuracy, billing practices, and documentation quality provide valuable feedback for improvement initiatives. External audits offer objective assessments and validation of internal controls.
Mastering revenue cycle processes requires coordinated efforts across multiple departments, systematic workflows, and continuous attention to performance metrics. Healthcare providers who optimize these processes experience improved cash flow, reduced administrative burden, and enhanced financial stability. Greenhive Billing Solutions delivers comprehensive revenue cycle management services that streamline operations from patient registration through final payment collection, ensuring maximum reimbursements while maintaining HIPAA compliance and transparent communication throughout every stage of the process.